Case Report
Indications and Results of Coronarography in Senegalese Diabetic Patients: About 45 Cases
Ndao SCT, Gaye ND*, Dioum M, Ngaide AA, Mingou JS, Ndiaye MB, Diao M and Ba SA
Cardiology Department, Aristide Le Dantec Teaching Hospital, BP: 6633 Dakar Etoile Dakar, Senegal
*Address for Correspondence: Gaye Ngone Diaba, Cardiology Department, Aristide Le Dantec Teaching Hospital, BP: 6633 Dakar Etoile Dakar, Senegal, Email: [email protected]
Dates: Submitted: 20 January 2017; Approved: 17 February 2017; Published: 20 February 2017
How to cite this article: Ndao SCT, Gaye ND, Dioum M, Ngaide AA, Mingou JS, et al. Indications and Results of Coronarography in Senegalese Diabetic Patients: About 45 Cases. J Cardiol Cardiovasc Med. 2017; 2: 013-019.
DOI: 10.29328/journal.jccm.1001007
Copyright License: © 2017 Ndao SCT, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Coronary angiography; Diabetic; Dakar
ABSTRACT
Introduction: Coronary disease accounts for 75% of diabetic mortality. Coronary angiography reveals lesions that are often diffuse, staggered and multi-truncated. The objective of this study was to determine the indications and results of coronary angiography in diabetic patients.
Method: This is a cross-sectional, descriptive and analytical study which took place from May 2013 to July 2015 at the cardiology clinic of the Aristide Le Dantec hospital. We have included all diabetics who have benefited from coronary angiography by studying clinical and paraclinical data, particularly coronary angiography ones.
Results: During this period, 400 patients had coronary angiography, including 45 diabetics, a hospital prevalence of 11.25%. The average age of our patients was 62.27 y/o with extremes of 44 and 85 y/o. The sex ratio was 1.6 in favor of men. Diabete was revealed in 42 patients. Almost all patients were type II diabetics (44 patients) since 9.94 years in average. The associated cardiovascular risk factors were hypertension 66.7% and dyslipidemia 49.6%. Only 4 patients had typical chest pain. The electrocardiogram was abnormal in 84.4% of cases with 26 cases of SCA ST +. Coronary angiography was abnormal in 37 patients with significant stenosis in 30 patients. A single-truncular lesion was found in 14 cases, 8 had bi-truncular and other 8 had tri-truncular one. The anterior interventricular artery and the segment II of the right coronary were the most affected branches. Concerning the management, 14 patients had angioplasty with an active stent, 8 patients had medical treatment alone and 9 patients had coronary artery bypass surgery. Accidents occured for 4 patients, two of whom had arterial spasm, one of a vagal discomfort and another had an occlusion of the circumflex that led to the implantation of a stent.
Conclusion: Diabetes is accompanied by progressive coronary atherosclerosis, which has an adverse effect on patients' prognosis. Tri-truncal affection and indications for coronary artery bypass surgery are common
INTRODUCTION
Diabetes is a dreadful metabolic disorder by its evolution, usually insidious, leading to a delayed diagnosis, resulting in patients exposure to complications, in particular cardiovascular complications [1]. It is a potent risk factor for coronary atherosclerosis and myocardial infarction [2]. Coronary disease is the leading cause of morbidity and mortality in diabetics [3].
It is clearly established that diabetic patients develop asymptomatic and yet often severe, diffuse, staged and multi-truncated coronary lesions [4].
Thus systematic screening for silent coronary artery disease in diabetic patients with high cardiovascular risk seems legitimate [5,6] especially in sub-Saharan Africa. Silent myocardial ischemia can be detected by non-invasive methods and, in case of positivity, coronary angiography will be performed for revascularization.
The objectives of our study were to specify the indications and describe the results of coronary angiography in diabetic patients in sub-Saharan Africa where this revascularization technique is in its beginnings.
METHODOLOGY
This is a cross-sectional study carried out at the Cardiology Clinic of the Aristide Le Dantec Hospital. It took place over a period of 4 years and 2 months from May 2013, corresponding to the start of coronary angiography activities, to July 2015.
All diabetic patients who had coronary angiography during this period were included. Data were collected on the basis of a survey including different parameters. The collection technique used was the questioning of the patients and the counting of their files.
Several parameters were studied, including socio-demographic, clinical and biochemical data. All patients also benefited from an electrocardiogram (ECG). Doppler echocardiography assessed the left ventricular systolic function by the Simpson biplane method, segmental and global kinetics. The left ventricular ejection fraction (LVEF) was considered to be slightly impaired if it was between 54 and 45%, moderately impaired between 44 and 30% and severely impaired by less than 30%.
At the angiographic level, the indications, the approach, the duration of the procedure, the dosimetry and the results had been specified. Elemental lesions, whether angiographically significant or not, were studied and evaluated according to the TIMI flow. We had investigated the affections of the common trunk, the mono, bi and tri truncular lesions. The incidents and accidents encountered during the proceedings had also been reported. The number of patients who had undergone angioplasty was specified, as was the technique used (direct stenting, pre-stent dilation plus stent, thrombo-aspiration), the type of stent used, the nature of the TIMI flow after angioplasty. All patients undergoing a percutaneous coronary intervention (PCI) were pretreated with a 600 mg dose of clopidogrel and 250 mg IV dose of aspirin. Patients with an indication of surgical revascularization or medical treatment alone were also sought.
The collected data were captured using an electronic questionnaire developed with SSPS version 17 softwares. Data analysis was performed using the same software. KHI 2 test and Fisher test were used for statistical purpose. The difference was considered statistically significant for a threshold of 5%. The odds ratio (OR) surrounded by its confidence interval was used to quantify the strength of the bond.
This study was approved by the Cheikh Anta DIOP university ethical comittee for research.
RESULTS
During this period, 400 patients had coronary angiography including 45 diabetics, thus a prevalence of 11.25%. There were 28 (62%) men and 17 (38%) women. The average age of patients was 62.27 years with extremes of 44 and 85 years. Hypertension was present in 29 patients (66.6%), dyslipidemia in 49.6% of cases. Figure 1 shows the distribution of patients according to cardiovascular risk factors.
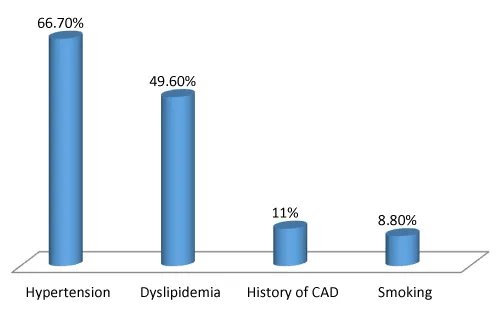
Figure 1: Repartition of patients according to cardiovascular risk factors.
Twenty (44.5%) patients had no other cardiovascular risk factors other than s and 33.3% of patients had at least one cardiovascular risk factor among high blood pressure (hypertension), Smoking, dyslipidemia and antecedent of coronary disease.
The diabetes hospital prevalence in coronary angiography patients was 11.25%. Diabetes was revealed in 93.3% (n=42), while 6.7% did not know they had diabetes (n=3). It was a type 2 diabete in 97.8% of cases. The average diabetes duration was 9.94 years (extremes of 28 days and 37 years). It was regularly monitored in 64.4% (n=29) of cases, irregularly followed in 17.8% and 8 patients were not on treatment (17.8%). Oral antidiabetic drugs (OAD) were used in 60% of cases (n=27). Six patients were under insulin and under diet alone (13.3%). In addition to coronary artery disease, three patients had already had a complication of diabetic macroangiopathy, two cases of stroke and one case of obliterative arteriopathy of the lower limbs.
Clinically, four patients (9%) had typical chest pain, nineteen patients (42.2%) had atypical pain and twenty-two (48.9%) were asymptomatic. Assymptomatic patients were mostly refered to cath lab because of a positive exerxise stress test. Dyspnea was present in 5 (11%) patients, two of whom were in stage III and IV respectively and one in stage II of the NYHA. The average blood sugar rate on an empty stomach was 2 g/l and the extremes were 0.61 and 4.46 g / l.
Twenty Eight (28) patients had a diabetic imbalance at admission (62.2%) and only nine patients had a normal rate (20%). The average glycated hemoglobin rate was 8.68% with extremes of 5.9 and 13.3%. Thirteen (28.9%) patients had a glycated hemoglobin level greater than 7%. Troponin I was positive in 37.8% (n=17). The average troponin I rate was 8.53 μg/l with extremes of 0.05 and 74.84 μg/l. Six patients had hypertriglyceridemia (13.3%),with an average value of 1.2 g/l, and extremes of 0.35 and 3.57 g/l. Hypercholesterolemia was found in 26.7% of patients and an increase of LDL cholesterol in 11.1% of cases.
The electrocardiogram was abnormal in 84.4% of the cases (n=38). Twenty-six patients (57.8%) had ST + coronary syndrome. The lower and antero-septo-apical territories were respectively reached in 13.3% of cases. Nine patients had sequelae of lower necrosis (20%) and seven of antero-septo-apical necrosis (15.6%). Three patients had right ventricular infarction (6.6%) and five had true posterior infarction (11.1%).
Table 1 summarizes the topographic forms of Acute Coronary Syndrome (ACS) at the ECG.
| Table 1: Topographic repartition of the acute coronary syndrom at electrocardiogram. | |||
| Territories | ST elevation | Non-ST elevation | Necrosis |
| Anteroseptal | 3 | 2 | 4 |
| Anteroseptal and apical | 6 | 1 | 7 |
| Extended anterior | 3 | 4 | 1 |
| High lateral | 2 | 5 | 0 |
| Down lateral | 1 | 7 | 0 |
| Inferior | 6 | 8 | 9 |
| Posterior | 1 | 1 | 5 |
| Right ventricle | 3 | 0 | 0 |
At echocardiography, left ventricular systolic function was normal in 64.4% (n=29), slightly altered in 6.7% (n=3), moderately altered in 24.4% (n=11) and severely altered in 4.4% (n=2).
Hypokinesia was the most frequent anomaly of the kinetics (76.7%) and the affection of the lower wall was predominant in 31.1% of cases.
Recent myocardial infarction was the first indication of coronary angiography (37.8%). The main indications of coronary angiography are summarized in table 2.
| Table 2: Repartition according on indications of coronary. | ||
| Indications | Number | Percentage (%) |
| Recent myocardial infarction | 17 | 37,8 |
| Unstable angina | 7 | 15,5 |
| Stable angina | 6 | 13,3 |
| Positive ischemia test | 4 | 8,9 |
| Non ST elevation myocardial infarction | 3 | 6,7 |
| Angina on ischemic cardiomyopathy | 3 | 6,7 |
| Residual angina after a previous myocardial infarction | 3 | 6,7 |
| Cardiogenic schock | 1 | 2,2 |
| Suspicion of restenosis | 1 | 2,2 |
The femoral pathway was used in 82.2%. Eight patients had a radial pathway (17.8%).
The average duration of the proceedings was 67 minutes. Minimum and maximum durations were 15 and 130 minutes.
The average of cumulative doses was 1023 cGy. The minimum dose was 155 cGy and the maximum dose was 4829 cGy. The average amount of contrast products used was 118 cc. The minimum quantity was 15 cc and the maximum was 1200 cc.
Coronary angiography was abnormal in 82.2% (n=37 patients). Thirty (30) had significant stenosis (66.6%) and 7 had a non-significant lesion (15.6%). Fourteen patients (31.1%) had significant mono-truncal affection. Significant bi-truncular and tri-truncular lesions were found in 8 patients (17.8%).
The distribution of the elemental lesions according to the coronary arteries is shown in table 3.
| Tables 3: Repartition of coronary artery lesions. | ||||||
| Coronary artery | Atheromatous | Non-significant lesion | Significant lesion | Occlusion | Number | Perentage (%) |
| TC | 7 | 0 | 2 | 0 | 9 | 20 |
| LAD1 | 4 | 2 | 9 | 3 | 18 | 40 |
| LAD2 | 3 | 3 | 12 | 3 | 21 | 46,7 |
| LAD3 | 1 | 1 | 4 | 1 | 7 | 15,6 |
| LCX1 | 6 | 2 | 4 | 2 | 14 | 31,1 |
| LCX2 | 1 | 0 | 3 | 0 | 4 | 8,9 |
| LCX3 | 3 | 1 | 7 | 2 | 13 | 28,9 |
| LMA1 | 0 | 0 | 1 | 0 | 1 | 2,2 |
| LMA 2 | 0 | 0 | 1 | 0 | 1 | 2,2 |
| RCA1 | 8 | 0 | 7 | 0 | 15 | 33,3 |
| RCA2 | 9 | 2 | 10 | 4 | 25 | 55,5 |
| RCA3 | 9 | 1 | 2 | 0 | 12 | 26,7 |
| PDA | 0 | 0 | 3 | 0 | 3 | 6,7 |
| PRA | 0 | 0 | 2 | 0 | 2 | 4,4 |
| LCA: Left coronary artery; LAD: Left anterior descending artery; LCX: Circumflex artery; LMA: Left marginal artery; RCA: Right coronary artery; PDA: Posterior descending artery; PRA: Posterior retroventricular artery. | ||||||
The figure 2 represents a coronary angiography image showing diffuse, multiple and tight lesions.
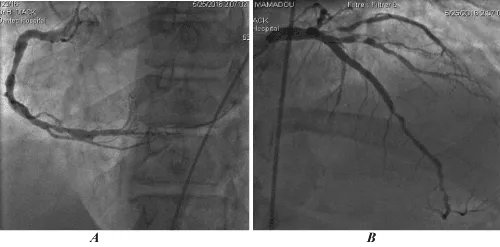
Figure 2: Image of coronary angiography by right femoral pathway showing diffuse, multiple and tight lesions. A (right coronary artery), B (left coronary artery).
Fourteen patients had angioplasty (31.1%). Drug eluting stents were used in all patients. One patient had thromboaspiration with stent placement. Balloon Pre-dilatation followed by stent placement was performed in 20% of cases, direct stenting in 8.8% and thrombo-aspiration followed by stenting in 2.2% of cases. All patients had TIMI 3 flow after angioplasty. Nine (9) patients had coronary artery bypass surgery (20%), and eight patients were referred for medical treatment (17.8%).
Thrombolysis was performed in three patients prior to coronary angiography (6.7%).
Three incidents were noted: two cases of pain in the right shoulder and a failure at angioplasty.
Accidents occured in 4 patients (8.9%): two cases of radial artery spasm which were successfully treated with IV nitrates, one case of vagal discomfort managed with IV atropine. One patient presented angina pain by iatrogenic dissection of the circumflex that motivated the placement of a stent.
Treatment with OAD was the only parameter correlated with the severity of coronary affection. Indeed, it appeared that none of the patients with a tritruncular lesion was treated with OAD (p=0.02).
On the other hand, there was no statistically significant correlation between the severity of coronary affection and other parameters such as age, gender, smoking, hypertension, dyslipidemia, type of diabetes follow-up, symptoms and electrocardiographic and echocardiographic abnormalities.
DISCUSSION
In our series, the hospital prevalence of diabetes in coronary insufficiency was 11.25%. It was roughly similar to literature data ranging from 10.9% to 20.3% [7].
We found a male predominance (62.2%) with a sex ratio of 1.6. This result is comparable to that found by CHAABANE and al (M/F ratio=1.32) [8].
The average age of coronary affection occurence in diabetics, relatively high (62.27 y/o), appears to be higher than in the literature, which varies from 52 to 60.7 y/o [7].
The average diabete duration was 9.94 years with extremes of 28 days and 37 years. It is comparable to that found by SOW (9.27 years) and slightly lower than that found by Chaâbane (12.57 years) [8]. The majority of our patients were regularly monitored (64.4%).
Recent myocardial infarction was the first indication for coronary angiography for our patients. It accounted for 37.8% of cases, followed by unstable angina (15.5%). Four patients had the indication of coronary angiography following the positivity of ischemic tests. The ischemia test used was the exertion test.
These results show the scarcity of silent ischemia detection in our medical practice. They prompt us to follow recommendations that suggest seeking silent ischemia through non-invasive exploration in high-risk diabetic patients.
Coronary angiography was abnormal in 82.2% of cases (n=37). The majority of the patients (66.6%) had a significant stenosis and in 15.6% of the patients the coronary lesion was insignificant. In our study, a mono-truncular stenosis was detected in 31.1% of the cases, also a double and tri-truncular stenosis, each in 17.8% of the cases. In the Guadeloupean population, ARMAND had found a mono-truncular lesion in 40.3%, a bi-truncular 25.3% and a tri-truncular 7.7% [9]. CHAABANE and al found a prevalence of 14% of tri-truncular stenosis, lower than our results [7].
However, several studies have shown the prevalence of multi-truncal affection in diabetics [9,10]. Only 14 (31%) patients received PCI. This small rate can be mostly explained by the lack of financial ressources to support the cost of the intervention. Complications rate in our study was 8,9%. Radial artery spasm and vagal malaise are common incidents during coronarography [11]. Coronary dissection is rare but potentially letal [12,13]. In our study, one patient experienced dissection of circumflexe artery which necessitaded angioplasty, due to utilization of rigid guiding catheters.
The bi-varied analysis made it possible to show that the absence of oral anti-diabetic treatment was a predictive factor of tri-truncular affection (p <0.02).
CONCLUSION
Diabetes is accompanied by progressive coronary atherosclerosis, which has an adverse effect on patients' prognosis. Tri-truncal affection and indications for coronary artery bypass surgery are common. Screening of silent myocardial ischemia is highly needed in diabetic population.
STUDY LIMITATIONS AND RECOMMENDATIONS
The main limitation of our study was the small sample size. These findings need to be replicated in larger prospective study in order to validate our results in black subsaharians african populations.
REFERENCES
- Bouzouba L, habbal R, De Poli F, Couppie P, Leddet P, et al. Syndrome coronarien aigu et diabète type 2 chez le sujet âgé. Ann Endocrinol. 2014; 75: 380-381. Ref.: https://goo.gl/lWP3UM
- Claude Le Feuvre. Coronary artery disease in patients with diabetes. Presse Med. 2009; 38: 964-972. Ref.: https://goo.gl/T1zGfv
- Dunning BE, Gerich JE. The role of alpha-cell dysregulation in fasting and postprandial hyperglycemia in type 2 diabetes and therapeutic implications. Endocr Rev. 2007; 28: 253-283. Ref.: https://goo.gl/oxoehA
- Tsujimoto T, Kajio H, Takahashi Y, Kishimoto M, Noto H, et al. Asymptomatic coronary heart disease in patients with type 2 diabetes with vascular complications: a cross-sectional study. BMJ Open. 2011; 1: 139. Ref.: https://goo.gl/SdqhsE
- Charbonnel B, Bouhanick B, Le Feuvre C. Recommendations of SPC/ALFEDIAM on the care of diabetic patient as seen by the cardiologist. Diabetes Metab. 2004; 30: S2-S24. Ref.: https://goo.gl/qo8BxL
- Muhlestein JB, Lappé DL, Lima JA, Rosen BD, May HT, et al. Effect of screening for coronary artery disease using CT angiography on mortality and cardiac events in high-risk patients with diabetes: the FACTOR-64 randomized clinical trial. JAMA. 2014; 312: 2234-2243. Ref.: https://goo.gl/4zJ4IH
- Turner RC, Millns H, Neil HA, Stratton IM, Manley SE, et al. Risk factors for coronary artery diseases in non-insulin dependent diabetes mellitus: United Kingdom Prospective Diabetes Study (UKPDS: 23). BMJ. 1998; 316: 823-828. Ref.: https://goo.gl/ZFCDpo
- Chaâbane A, Rekik N, Graja S, Mnif M, Abid M. Caractéristiques épidémiologiques, cliniques et thérapeutiques de la coronaropathie chez les patients diabétiques au service d’endocrinologie-diabétologie, CHU Hédi Chaker, Sfax, Tunisie. Diabetes Metab. 2013; 39: 72. Ref.: https://goo.gl/aX374N
- Armand L, Larifla FL, Velayoudom J, Deloumeaux J, Weladji G, et al. Coronaropathie et diabète dans la population guadeloupéenne. Diabetes Metab. 2012; 38: 40. Ref. https://goo.gl/rvlIwJ
- Goraya TY, Leibson CL, Palumbo PJ, Weston SA, Killian JM, et al. Coronary atherosclerosis in diabetes mellitus: a population-based autopsy study. J Am Coll Cardiol. 2002; 40: 946-953. Ref.: https://goo.gl/R1XKVI
- Trilla M, Freixa X, Regueiro A, Fernández-Rodriguez D, Brugaletta S, et al. Impact of Aging on Radial Spasm During Coronary Catheterization. J Invasive Cardiol. 2015; 27: 303-307. Ref.: https://goo.gl/dfXWwd
- Djenić N, Dzudović B, Romanović R, Ratković N, Jović Z, et al. Iatrogenic dissection of the left main coronary artery during elective diagnostic procedures--A report on three cases. Vojnosanit Pregl. 2016; 73: 284-287. Ref.: https://goo.gl/1JVK1r
- Barber-Chamoux N, Souteyrand G, Combaret N, Ouedraogo E, Lusson JR, et al. Contribution of optical coherence tomography imaging in management of iatrogenic coronary dissection. Cardiovasc Revasc Med. 2016; 17: 138-142. Ref.: https://goo.gl/jgGH5O