
More Information
Submitted: November 11, 2022 | Approved: November 21, 2022 | Published: November 22, 2022
How to cite this article: Habib M. Acute ischemic stroke for alteplase or medical care alone or intervention with/without alteplase in Palestine (AIS-AMI Palestine). J Cardiol Cardiovasc Med. 2022; 7: 093-097.
DOI: 10.29328/journal.jccm.1001140
Copyright License: © 2022 Habib M. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Acute ischemic stroke for alteplase or medical care alone or intervention with/without alteplase in Palestine (AIS-AMI Palestine)
Mohammed Habib*
MD, Ph.D, Head of Cardiology Department, Alshifa Hospital, Gaza, Palestine
*Address for Correspondence: Mohammed Habib, MD, Ph.D, Head of Cardiology Department, Alshifa Hospital, Gaza, Palestine, Email: [email protected]
Background: Stroke is the most common cause of permanent disability and the third most common cause of death in Palestine. We aimed to examine patterns of stroke presentation, causes, management and outcomes at the largest public Mistry of health hospitals in Palestine.
Methods: Comprehensive data from all patients with acute ischemic stroke who were admitted to al-Shifa hospital between November 2021 and July 2022 and treated with alteplase alone or endovascular intervention with or without alteplase were prospectively collected and compare with acute ischemic stroke patients who were treated with medical care alone at Palestine medical complex hospital at 2018. Acute ischemic stroke presentation patterns, in-hospital evaluation and management, mortality, and morbidity were evaluated.
Results: Medical care alone group: 138 patients with acute ischemic stroke, mean age was 65 ± 14 years and 49% were women. Most of the patients received antiplatelet therapy (98%), although none received thrombolysis. Only 17% received physical therapy evaluation. In-hospital mortality was 13%, and a modified ranking score of 0 -2 was in 44 patients (32%). Endovascular intervention with/without alteplase group: 56 patients with acute ischemic stroke. The mean age was 61 ± 12 years and 41% were women. All patients received brain computed tomography scans, although few received other investigations such as carotid Doppler (13%). Most patients with ischemic stroke received antiplatelet therapy (99%), although 39 patients (70%) received thrombolysis. Only 61% received physical therapy evaluation. In-hospital mortality was 7%. The modified ranking score 0 - 2: 32 patients (57%).
Conclusion: This study conducted in Palestine showed that among patients with acute ischemic stroke, functional outcomes according to modified ranking score 0 - 2 were better by endovascular therapy with/without alteplase than with medical care alone.
Stroke is one of the leading causes of death and disability worldwide. The tissue Plasminogen Activator (tPA) is the only therapeutic agent approved to treat patients with acute ischemic stroke [1]. According to the American Heart Association/American Stroke Association Guidelines for the Early Management of Patients with Acute Ischemic Stroke the clinical benefits of tPA manifest when the agent is administered within 4.5 hours of stroke onset [2]. However, intravenous (IV) tPA administration is associated with an increased occurrence of intracranial hemorrhage [3-5]. Each year in Palestine, approximately 5200 people have an acute ischemic stroke. About 12% of mortality is related to stroke [6]. On average, every 75 minutes, someone in Palestine has a stroke, and every 6 hours one Palestinian died from a stroke. The intravenous tPA was started to treat acute ischemic stroke in Palestine in 2000. Before this time all patients treated with medical care alone (antiplatelet, statin, antihypertensive, antidiabetic, and physiotherapy) before modern treatments at Palestine in-hospital mortality between 1 - 5 days was 13% and among survivors, more than 60% of patients had moderate-to-severe neurologic deficits [7]. The introduction of intravenous alteplase in 1995 led to substantial improvement in outcomes [8]. More recently, effective mechanical throm-bectomy has radically altered initial management in many patients. The thrombolytics treatment with tPA and mechanical thrombectomy was started in the Gaza strip for acute ischemic stroke in November 2021.
Study design and settings
Four major healthcare providers exist in Palestine: the Palestinian Ministry of Health, Palestinian nongovernmental organizations, the United Nations Relief, and the private sector. Secondary and tertiary care is mostly provided through the Ministry of Health in 12 hospitals distributed in the West Bank and in 13 hospitals in the Gaza strip for the old treatment strategy, we purposively sampled 2 of the largest Ministry of Health hospitals in the West Bank. Palestine Medical Complex Hospital in Ramallah City is located in the Center and had 231 beds, serving a population of 338 383 residents. Al-Watani Hospital in Nablus City is located in the North and has 255 beds, serving a population of 372 621 residents.
For the new treatment strategy, the sample is collected from the largest hospital in Palestine and located in Gaza city which has 600 beds, serving 722350 residents.
At the time of data collection, acute stroke was managed by internal medicine specialists and a neurologist at the Palestine Medical Complex Hospital and Al-Shifa hospital. Al-Watani Hospital did not have a neurology specialist at the time of data collection and acute stroke was managed by internal medicine specialists.
Data were collected between September 2017 and May 2018 from Palestine Medical Complex Hospital and between February 2018 and May 2018 from Al-Watani Hospital. And between November 2021 and July 2022 from Al-Shifa Hospital.
The data, analytic methods, and study materials will not be made available to other researchers for the purposes of reproducing the results or replicating the procedure.
The present prospective registry study involved all patients with acute ischemic stroke who were admitted to al-Shifa hospital between November 2021 and July 2022 and treated with alteplase alone or endovascular intervention with/without alteplase were prospectively collected (new treatment strategy) And compared with acute ischemic stroke patients who treated with medical care alone at West Bank (Palestine medical complex hospital and Alwatani hospital) at 2018 (before the beginning of the administration of IV tPA or mechanical thrombectomy in Palestine) (old treatment strategy).
he old treatment strategy (medical care alone) [7]
Involved 138 patients, a prospective hospital-based registry at hospitals in the West Bank of Palestine, the stroke management including medical care alone (absence of thrombolytic therapy and endovascular intervention).
The new treatment strategy (endovascular intervention with or without tPA or Tpa alone)
Eligibility criteria included receipt of intravenous t-PA (0.6 mg per kilogram), with 15% as a bolus and the remainder infused over a 1-hour period (maximum dose, 60 mg) within 4.5 hours after symptom onset and moderate-to-severe neurologic deficit according to the National Institutes of Health Stroke Scale (defined as an NIHSS score ≥ 6). For patients with suspicion of large vessel occlusion (NIHSS ≥ 6 or RACE score ≥ 5 or VAN positive) [8,9], the angiographic procedure had to begin before finishing the T-PA infusion and be completed within 6 hours (5 - 7 hours) after the onset of stroke. Or if t-PA is contraindicated the patient is transferred directly to the cardiac catheterization laboratory. Participants who had no angiographic evidence of a treatable occlusion received no additional treatment, and those with a treatable vascular occlusion received endovascular intervention with an approach chosen by the site (i.e., thrombectomy with aspiration catheter or endovascular delivery of Intraarterial alteplase (maximum dose, 30 mg) by means of the standard microcatheter). Heparin infusion was started intravenously with a 5000-unit bolus, followed by an infusion of 1000 units per hour if endovascular therapy is more than 1 hour, and was discontinued at the end of the procedure. CT was performed at baseline, at 24 hours (± 6 hours), and if there was a neurologic decline. Written informed consent was obtained from the patient (Figure 1).
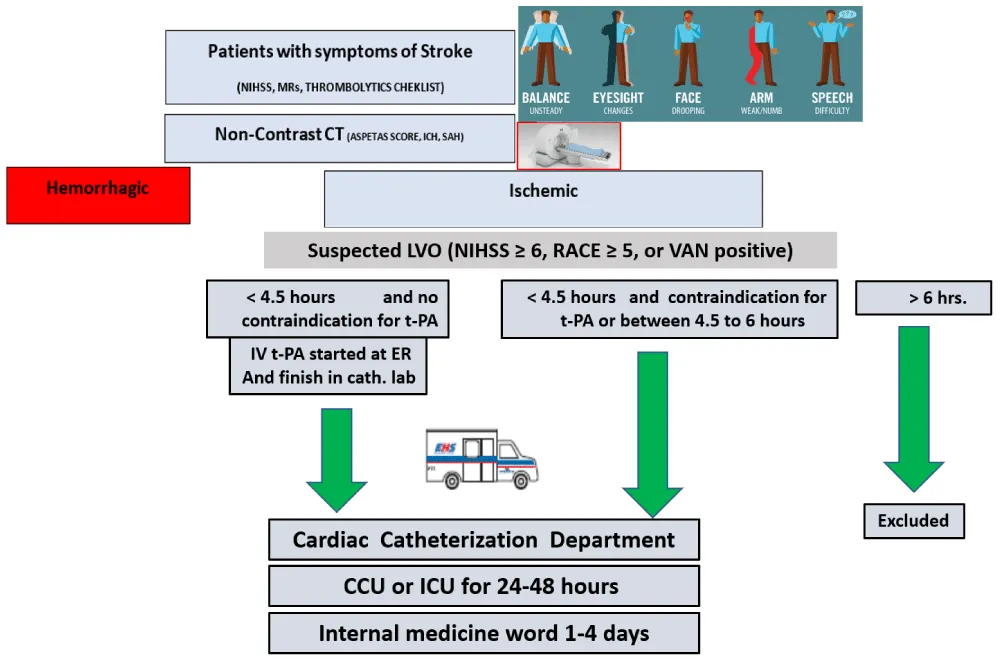
Figure 1: Chart of a new treatment strategy for acute ischemic stroke in al-Shifa hospital in Gaza. CCU: Coronary Care Unit; ICU: Intensive Care Unit; NIHSS: National Institutes of Health Stroke Scale; RACE: Rapid Arterial occlusion Evaluation (RACE) Scale for Stroke; VAN: Stroke vision, aphasia, neglect (VAN) assessment).
The primary outcome (Discharge outcomes)
At discharge, was the score on the modified Rankin scale assessed and death at the time of hospital discharge?
Statistical analysis
Continuous data are reported as means ± SD where appropriate. Categorical data are presented as absolute values and percentages. Statistical analyses were performed by X square test to compare the primary outcome(modified Rankin scale 0 - 2 and death) between medical care alone and new treatment strategy involved tPA and endovascular intervention or between medical care alone and a p - value < 0.05 was considered significant.
The old treatment strategy [7]
The mean age (SD) was 65 ± 14 years and 49% were women. Only 25% of patients arrived by emergency medical services and 61% arrived at the hospital within 3 hours of symptom onset, of whom 57% received imaging within 45 minutes of arrival. Most strokes were ischemic (92%). Patients were most commonly admitted to the medical unit (84%), while 13% were admitted to the intensive care unit or the cardiac care unit. All patients received head computed tomography scans, although few received other investigations such as magnetic resonance imaging (8%) or carotid Doppler (4%). Most patients with ischemic stroke received antiplatelet therapy (98%), although none received thrombolysis. Only 17% received physical therapy evaluation. In-hospital mortality was 12%. The median National Institutes of Health Stroke Scale was 8.5 (4 - 15). Hypertension was the most common risk factor reported by 67% of patients. 23% of patients had at least 1 poststroke complication, and the median modified Rankin Score at discharge was 4 (interquartile range, 2 - 5). At discharge, the median modified Rankin Scale score of 0 - 2 was in 44 patients (32%), moderate to severe disabilities were seen in 61% of patients and 13% of patients died during the hospital stay. We also identified several gaps in acute stroke management including the absence of thrombolytic therapy and endovascular intervention, low rates of diagnostic vascular and cardiac imaging, and limited rehabilitation services.
The new treatment strategy
Total number of patients from November 2021 and July 2022 who were admitted to al-Shifa hospital and treated by intravenous tPA and/or endovascular treatment was 56 patients, with a mean age was 61 ± 12 years and 41% were women. Cause of stroke: Cardio-embolism: 26(46%), Intracranial atherosclerosis: 5 (9%) Ipsilateral extracranial ICA obstruction: 4(7%), Undetermined: 21(38%), the median ASPECTS score was 7 - 10 [9]. Symptomatic intracranial hemorrhage within 48 hours was seen in 4 (7%), intrahospital death was seen in 4 cases (7%), 3 cases in t-PA(16.6%), 1(3%)case in endovascular intervention with tPA (3%)and no mortality in intervention alone. Modified Rankin scale score of 0 to 2 at discharge in 32 patients (57%), 25 patients in the intervention group, and 7 in patients who received alteplase.
Patients are divided into 2 groups
1. Intervention with/without tPA (38 patients 68%): A total of 17 (30%) patients were assigned to undergo endovascular treatment and 21 (38%) were assigned to receive combination therapy with intravenous alteplase and endovascular treatment.
2. tPA alone (18 patients, 32%): Patients receive intravenous alteplase alone Baseline characteristics of the patients in old and new treatment strategies in acute ischemic stroke are in Table 1.
| Table 1: Characteristics of the Patients at Baseline. | ||
| Characteristics | New treatment strategy 56 patients |
Old treatment strategy 138 patients |
| Age (mean) | 61 ± 12 years | 65 ± 14 years |
| Male | 33 (59%) | 72 (52%) |
| Median NIHSS score | Mild (NIHSS 0 - 6):12(21%) Moderate (NIHSS 7 - 12): 29(52%) Severe (NIHSS > 13):15(27%) |
Mild (NIHSS 0 - 6):53(38%) Moderate (NIHSS 7 - 12): 41(30%) Severe (NIHSS 13 - 20):44(32%) |
| Medical history Previous ischemic stroke History of atrial fibrillation History of diabetes mellitus History of hypertension |
11(20%) 19(34%) 21(37%) 29(52%) |
54(39%) 26(19%) 63(46%) 91(66%) |
| NIHSS: National Institutes of Health Stroke Scale | ||
Primary outcome (Discharge outcomes)
At discharge, the modified ranking score between 0-2 was more in new treatment strategy was seen in 32 (57%) of patients in the new treatment strategy and in 44 patients (32%) in the old treatment strategy (P:001), intra-hospital death in 4 (7%) of patients in new treatment strategy and in 18(13%) of patients in old treatment strategy (P:0.2) Table 2.
| Table 2: Primary outcome in new and old treatment strategy. | |||
| New treatment strategy | Old treatment strategy | p value | |
| mRS 0-2 | 32 | 44 | 0.001 |
| Intra hospital death | 4 | 18 | 0.2 |
| mRS: modified ranking score | |||
omparison between Intervention with/out tPA and old treatment strategy
Modified ranking score between 0-2 was seen in 25 (66%) of a patient who undergo endovascular intervention with or without tPA and in 44 (32%) of a patient with old treatment strategy (P:0001) and intra-hospital death in one patient’s mortality who undergo endovascular intervention with tPA and in 18 (13%) of patients with old treatment strategy(P:0027) Table 3.
| Table 3: Primary outcome in Intervention with/without tPA and old treatment strategy. | |||
| (Endovascular ± tPA) | Old treatment strategy | p value | |
| mRS 0-2 | 25 | 44 | 0.0001 |
| Intra hospital death | 1 | 18 | 0.0027 |
| mRS: Modified Ranking Score | |||
Comparison between tPA alone and old treatment strategy
No significant difference between mRS 0 - 2 or mortality at hospital discharge between the two groups.
In this prospective hospital-based registry at public hospitals in the West Bank and Gaza strip of Palestine, we observed high rates of discharge disability and mortality. We also identified several gaps in acute stroke management including the absence of thrombolytic therapy, low rates of diagnostic vascular and cardiac imaging, and limited rehabilitation services in 2018 in west bank public hospitals.
After starting intravenous tPA plus endovascular intervention for acute ischemic stroke At Al-Shifa hospital in Gaza in 2021 we observed improvement in disability and a significant reduction of intra-hospital death when we treated acute ischemic stroke by a combination of alteplase and endovascular treatment.
The benefit of intravenous alteplase is time-dependent. In a meta-analysis of nine randomized, controlled trials [10], 32.9% of the patients in the alteplase group, as compared with 23.1% of the patients in the control group, had a favorable 3-month outcome (defined as a modified Rankin scale score of 0 or 1) when treatment was administered within 3 hours after the onset of stroke, the corresponding rates were 35.3% and 30.1% when treatment was administered between 3 and 4.5 hours after onset. Large intracerebral hemorrhage occurred in 6.8% of the patients in the alteplase group and in 1.3% of those in the control group. The overall outcomes, as assessed by the modified Rankin scale, among the patients in the alteplase group reflected the deleterious effects of hemorrhage along with the beneficial effect on ischemic stroke recovery. In our study, only 18 patients had received alteplase alone, and a total of 3 patients died, 2 patients of these died because of large intracerebral hemorrhage and one died because of administration of alteplase in large ischemic stroke with an NIHSS score was 26.
Pooled data from five randomized, controlled trials showed that the percentage of patients who had a modified Rankin scale score of 0 to 2 at 90 days was higher among those who underwent mechanical thrombectomy than among those who did not (46.0% vs. 26.5%) [11]. A randomized, controlled noninferiority trial that compared mechanical thrombectomy alone with the combination of intravenous alteplase and mechanical thrombectomy in patients eligible for both interventions met its large prespecified noninferiority margin (the modified Rankin scale score with thrombectomy alone at 90 days was less than 20% worse than that with combined therapy); the adjusted odds ratio was 1.07 [12] Direct aspiration as the first approach for thrombectomy has been shown to be non-inferior to stent retrievers [13]. In our trial Intervention with/out tPA was administrated in 38 patients, 17 patients were assigned to undergo endovascular treatment alone and 21 were assigned to receive combination therapy with intravenous alteplase and endovascular treatment. One patient died after tPA because of tandem stroke and a modified Rankin scale score of 0 to 2 was in 25 patients.
Our results provide insight into the management and outcomes of patients with stroke in Palestine can be improved if we support a new treatment strategy with intravenous tPA within 4.5 hours and endovascular intervention with 6 hours of symptoms. These results highlight 4 areas to focus on to improve acute stroke care in public hospitals: (1) develop an organized stroke unit within a geographically defined location in each hospital and identify a multidisciplinary stroke team comprising medical, nursing, physiotherapy, occupational therapy, speech therapy, and social work staff. Given the limited resources, a stroke unit may comprise a set number of beds within an already established medical unit or intensive care unit; (2) support acute thrombolysis with intravenous tissue-type plasminogen activator and endovascular intervention (3) raise awareness in the community about recognition of stroke symptoms (4) implement a pathway for early discharge planning in the hospital. Early discharge planning strategies include early assessment of discharge needs, identification of realistic rehabilitation recovery goals, involving the patient and their family in the recovery process, and early rehabilitation at home or in the community.
We describe stroke presentation, management, and outcomes in public hospitals in Palestine. Results indicate poor clinical outcomes at discharge including high mortality rates and severe disability in medical care alone and improvement of disability and mortality by treatment of the combination of intravenous alteplase and endovascular intervention.
- National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group Tissue plasminogen activator for acute ischemic stroke. N Engl J Med. 1995; 333:1581–1587.
- Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, Biller J, Brown M, Demaerschalk BM, Hoh B, Jauch EC, Kidwell CS, Leslie-Mazwi TM, Ovbiagele B, Scott PA, Sheth KN, Southerland AM, Summers DV, Tirschwell DL. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2019 Dec;50(12):e344-e418. doi: 10.1161/STR.0000000000000211. Epub 2019 Oct 30. Erratum in: Stroke. 2019 Dec;50(12):e440-e441. PMID: 31662037.
- Emberson J, Lees KR, Lyden P, Blackwell L, Albers G, Bluhmki E, Brott T, Cohen G, Davis S, Donnan G, Grotta J, Howard G, Kaste M, Koga M, von Kummer R, Lansberg M, Lindley RI, Murray G, Olivot JM, Parsons M, Tilley B, Toni D, Toyoda K, Wahlgren N, Wardlaw J, Whiteley W, del Zoppo GJ, Baigent C, Sandercock P, Hacke W; Stroke Thrombolysis Trialists' Collaborative Group. Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: a meta-analysis of individual patient data from randomised trials. Lancet. 2014 Nov 29;384(9958):1929-35. doi: 10.1016/S0140-6736(14)60584-5. Epub 2014 Aug 5. PMID: 25106063; PMCID: PMC4441266.
- Lees KR, Emberson J, Blackwell L, Bluhmki E, Davis SM, Donnan GA, Grotta JC, Kaste M, von Kummer R, Lansberg MG, Lindley RI, Lyden P, Murray GD, Sandercock PA, Toni D, Toyoda K, Wardlaw JM, Whiteley WN, Baigent C, Hacke W, Howard G; Stroke Thrombolysis Trialists’ Collaborators Group. Effects of Alteplase for Acute Stroke on the Distribution of Functional Outcomes: A Pooled Analysis of 9 Trials. Stroke. 2016 Sep;47(9):2373-9. doi: 10.1161/STROKEAHA.116.013644. Epub 2016 Aug 9. PMID: 27507856; PMCID: PMC5024752.
- Goyal M, Menon BK, van Zwam WH, Dippel DW, Mitchell PJ, Demchuk AM, Dávalos A, Majoie CB, van der Lugt A, de Miquel MA, Donnan GA, Roos YB, Bonafe A, Jahan R, Diener HC, van den Berg LA, Levy EI, Berkhemer OA, Pereira VM, Rempel J, Millán M, Davis SM, Roy D, Thornton J, Román LS, Ribó M, Beumer D, Stouch B, Brown S, Campbell BC, van Oostenbrugge RJ, Saver JL, Hill MD, Jovin TG; HERMES collaborators. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet. 2016 Apr 23;387(10029):1723-31. doi: 10.1016/S0140-6736(16)00163-X. Epub 2016 Feb 18. PMID: 26898852.
- Palestinian Ministry of Health. Health Annual Report Palestine 2020. obtained from the Ministry of Health's website. www.moh.ps
- Khatib R, Jawaadah AM, Khammash U, Babiker A, Huffman MD, Prabhakaran S. Presentation, Management, and Outcomes of Acute Stroke in Palestine. J Am Heart Assoc. 2018 Nov 20;7(22):e010778. doi: 10.1161/JAHA.118.010778. PMID: 30571480; PMCID: PMC6404450.
- Pérez de la Ossa N, Carrera D, Gorchs M, Querol M, Millán M, Gomis M, Dorado L, López-Cancio E, Hernández-Pérez M, Chicharro V, Escalada X, Jiménez X, Dávalos A. Design and validation of a prehospital stroke scale to predict large arterial occlusion: the rapid arterial occlusion evaluation scale. Stroke. 2014 Jan;45(1):87-91. doi: 10.1161/STROKEAHA.113.003071. Epub 2013 Nov 26. PMID: 24281224.
- Teleb MS, Ver Hage A, Carter J, Jayaraman MV, McTaggart RA. Stroke vision, aphasia, neglect (VAN) assessment-a novel emergent large vessel occlusion screening tool: pilot study and comparison with current clinical severity indices. J Neurointerv Surg. 2017 Feb;9(2):122-126. doi: 10.1136/neurintsurg-2015-012131. Epub 2016 Feb 17. PMID: 26891627; PMCID: PMC5284468.
- Thomalla G, Simonsen CZ, Boutitie F, Andersen G, Berthezene Y, Cheng B, Cheripelli B, Cho TH, Fazekas F, Fiehler J, Ford I, Galinovic I, Gellissen S, Golsari A, Gregori J, Günther M, Guibernau J, Häusler KG, Hennerici M, Kemmling A, Marstrand J, Modrau B, Neeb L, Perez de la Ossa N, Puig J, Ringleb P, Roy P, Scheel E, Schonewille W, Serena J, Sunaert S, Villringer K, Wouters A, Thijs V, Ebinger M, Endres M, Fiebach JB, Lemmens R, Muir KW, Nighoghossian N, Pedraza S, Gerloff C; WAKE-UP Investigators. MRI-Guided Thrombolysis for Stroke with Unknown Time of Onset. N Engl J Med. 2018 Aug 16;379(7):611-622. doi: 10.1056/NEJMoa1804355. Epub 2018 May 16. PMID: 29766770.
- Goyal M, Menon BK, van Zwam WH, Dippel DW, Mitchell PJ, Demchuk AM, Dávalos A, Majoie CB, van der Lugt A, de Miquel MA, Donnan GA, Roos YB, Bonafe A, Jahan R, Diener HC, van den Berg LA, Levy EI, Berkhemer OA, Pereira VM, Rempel J, Millán M, Davis SM, Roy D, Thornton J, Román LS, Ribó M, Beumer D, Stouch B, Brown S, Campbell BC, van Oostenbrugge RJ, Saver JL, Hill MD, Jovin TG; HERMES collaborators. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet. 2016 Apr 23;387(10029):1723-31. doi: 10.1016/S0140-6736(16)00163-X. Epub 2016 Feb 18. PMID: 26898852.
- Yang P, Zhang Y, Zhang L, Zhang Y, Treurniet KM, Chen W, Peng Y, Han H, Wang J, Wang S, Yin C, Liu S, Wang P, Fang Q, Shi H, Yang J, Wen C, Li C, Jiang C, Sun J, Yue X, Lou M, Zhang M, Shu H, Sun D, Liang H, Li T, Guo F, Ke K, Yuan H, Wang G, Yang W, Shi H, Li T, Li Z, Xing P, Zhang P, Zhou Y, Wang H, Xu Y, Huang Q, Wu T, Zhao R, Li Q, Fang Y, Wang L, Lu J, Li Y, Fu J, Zhong X, Wang Y, Wang L, Goyal M, Dippel DWJ, Hong B, Deng B, Roos YBWEM, Majoie CBLM, Liu J; DIRECT-MT Investigators. Endovascular Thrombectomy with or without Intravenous Alteplase in Acute Stroke. N Engl J Med. 2020 May 21;382(21):1981-1993. doi: 10.1056/NEJMoa2001123. Epub 2020 May 6. PMID: 32374959.
- Turk AS 3rd, Siddiqui A, Fifi JT, De Leacy RA, Fiorella DJ, Gu E, Levy EI, Snyder KV, Hanel RA, Aghaebrahim A, Woodward BK, Hixson HR, Chaudry MI, Spiotta AM, Rai AT, Frei D, Almandoz JED, Kelly M, Arthur A, Baxter B, English J, Linfante I, Fargen KM, Mocco J. Aspiration thrombectomy versus stent retriever thrombectomy as first-line approach for large vessel occlusion (COMPASS): a multicentre, randomised, open label, blinded outcome, non-inferiority trial. Lancet. 2019 Mar 9;393(10175):998-1008. doi: 10.1016/S0140-6736(19)30297-1. PMID: 30860055.