
More Information
Submitted: June 18, 2024 | Approved: June 28, 2024 | Published: June 29, 2024
How to cite this article: Maloof A, Barba DT, Nuño SR, Bains NK, Zepeda IA, et al. Improving Cardiac Rehabilitation Referral Rates in Patients with Coronary Heart Disease from Diverse Communities Using an Electronic Order System. J Cardiol Cardiovasc Med. 2024; 9: 102-109. Available from: https://dx.doi.org/10.29328/journal.jccm.1001187
DOI: 10.29328/journal.jccm.1001187
Copyright License: © 2024 Akmal S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Coronary heart disease; Cardiac rehabilitation; Electronic order set; Disparities; Race and ethnicity
Abbreviations: EOS: Electronic Order Set; CR: Cardiac Rehabilitation; PCI: Percutaneous Coronary Intervention; CABG: Coronary Artery Bypass Grafting; MI: Myocardial Infarction; LVEF: Left Ventricular Ejection Fraction; COPD: Chronic Obstructive Pulmonary Disease; OR: Odds Ratio; CI: Confidence Interval; ACS: Acute Coronary Syndrome; CHD: Coronary Heart Disease

Improving Cardiac Rehabilitation Referral Rates in Patients with Coronary Heart Disease from Diverse Communities Using an Electronic Order System
Alexandra Maloof1,2*, David Torres Barba1,3, Santiago Ramirez Nuño3, Nainjot K Bains4, Ignacio A Zepeda5, Armando Gallegos1, Hyeri You6, Wesley Thompson6, Jia Shen1,3, Robert El-Kareh1,7 and Luis R Castellanos1,3
1University of California San Diego School of Medicine, La Jolla, California, USA
2Baylor College of Medicine, Houston, Texas, USA
3University of California San Diego Department of Medicine, Division of Cardiovascular Medicine and Sulpizio Family Cardiovascular Center, La Jolla, California, USA
4University Health Sciences Southern California Medical Education Consortium, Temecula, California, USA
5Sarver Heart Center, University of Arizona, Tucson, Arizona, USA
6Altman Clinical and Translational Research Institute (ACTRI), La Jolla, California, USA
7University of California San Diego, Department of Medicine, Division of Biomedical Informatics, USA
*Address for Correspondence: Alexandra Maloof, University of California San Diego School of Medicine, La Jolla, California, Baylor College of Medicine, Houston, Texas, USA, Email: [email protected]
Introduction: Despite the benefits of Cardiac Rehabilitation (CR), local and national CR referral and participation rates remain low when compared to established cardiovascular therapies, especially amongst racial/ethnic groups.
Objectives: This study investigated the effects of the implementation of a CR program and electronic order set (EOS) in a large health system on CR referral and participation rates among a diverse group of patients with Coronary Heart Disease (CHD).
Methods: A total of 360 patients from UCSD Health who presented with ACS were prospectively evaluated during initial hospitalization and 6- and 12-weeks post-discharge. The multivariable logistic regression model assessed referral and participation rates by week 1 and -12 post-discharge, adjusting for gender, age, race, ethnicity, geography, and referring physician subspecialty.
Results: UCSD CR program implementation led referral rates to increase at week 1 (Pre- 38.6% and Post-54.9%, p = 0.003) and week-12 (Pre- 54.1% and Post- 59.8%, p = 0.386). Post-CR referrals were more likely at week-1 (OR: 1.93, 95% CI 1.27-2.95) and week-12 (OR: 1.26, 95% CI 0.79-2.00). EOS implementation increased referral rates at week-1 (Pre- 40.3% and Post- 58.7%, p < 0.001) and week-12 (Pre- 54.9% and Post- 60.4%, p = 0.394) with referrals more likely at week-1 (OR: 2.1, 95% CI 1.35-3.29) and week-12 (OR: 1.25, 95% CI 0.795-1.98). Participation in CR following EOS was more likely at both week-1 and week-12. Multivariable analysis revealed disparities in referral based on race, geographic location, and referring physician subspecialty.
Conclusion: A CR program and EOS implementation were shown to increase referral rates with long-term potential for increasing referral and participation rates.
Condensed abstract: This prospective study investigated the implementation of a Cardiac Rehabilitation (CR) program and Electronic Order Set (EOS) within the same health system on CR referral and participation rates. 360 patients with ACS were evaluated over 12 weeks. UCSD CR program and EOS implementation led referral rates to increase at week-1 and -12. CR participation was more likely to increase at week-1 and -12 following EOS. Multivariable analysis revealed disparities in referrals disproportionally affecting racial and ethnic minority groups and rural communities. CR and EOS implementation may increase CR referral rates for diverse patients with CHD.
Cardiac Rehabilitation (CR) is a medically supervised preventative cardiovascular program that involves a multi-disciplinary approach including physician-prescribed exercises, cardiac risk factor modification (education, counseling, and behavioral intervention), psycho-social assessment, outcomes assessment, and individual treatment plans [1,2]. It is recommended for both inpatient and outpatient settings following cardiovascular illnesses including Myocardial Infarction (MI), Percutaneous Coronary Intervention (PCI), coronary artery bypass grafting (CABG), and for those with documented chronic stable angina [2].
The benefits of CR are well-studied and participation is considered a Class Ia recommendation by the American Heart Association (AHA) and American College of Cardiology (ACC) for patients with coronary heart disease (CHD) including acute MI or coronary revascularization [3,4]. Despite the documented benefits, referral and participation rates are strikingly low. Suaya, et al. [5] found CR utilization ranges from 5.2% to 42% across states, and Ades, et al. [6] noted low CR participation rates, ranging from 19% to 34% in national analyses.
The AHA Get with the Guidelines tool [7] is an electronic program designed to facilitate referrals and maximize inpatient quality improvement. This “automatic” referral strategy raises awareness regarding CR eligibility and ensures physicians consider CR as part of the integral process for patient recovery and overall wellness. Availability and use of an Electronic Ordering System (EOS) have been suggested to possibly improve CR utilization [8,9]. Therefore, we set to investigate the effects of the availability of both a local CR program and an EOS on referral and participation rates within a diverse patient population with CHD. We hypothesized that the availability of a local CR program and EOS would positively impact referrals and optimally reflect enrollment and participation rates.
Study design and population
Our prospective study included 360 patients hospitalized with ACS in the quaternary hospitals part of UCSD Medical Center and the UCSD Sulpizio Cardiovascular Center. Inclusion criteria included adult patients ≥ 18 years from rural and urban communities admitted for PCI, CABG, or acute MI who were able to provide written informed consent before initiation of the study and who displayed fluency in written English, Spanish, or Chinese. Additional inclusion criteria included access to a telephone, availability of baseline health status data, and achievement of clinical stability allowing study participation, specifically cardiac rehabilitation. A key factor for selecting patients was enrolling patients within one week of an acute coronary event or qualifying cardiac procedure and ensuring the ability to ambulate. Exclusion criteria included decompensated congestive heart failure (NYHA III or IV) at the time of enrollment, LVEF ≤ 35%, and any of the following comorbid medical conditions; severe COPD, need for additional cardiac revascularization procedure, severe peripheral arterial disease, uncontrolled arrhythmias, stroke within 6 months of enrollment, significant anemia (hemoglobin <9 mg/dL), active drug use and life expectancy less than 1 year.
Hospitalized patients enrolled in the study were asked to answer a survey at the time of discharge (week 1) and received follow-up phone calls six and twelve weeks following their discharge to complete additional surveys (Figure 1). CR referral, enrollment, and participation rates were determined based on information provided in patient surveys. For this study, week 1 and week 12 surveys were included in the analysis. The period investigated was between 5/27/2015 to 4/23/2019, during which the implementation of the UCSD CR program (est. January 2018) and the EOS (est. June 2018) were studied. There were 360 eligible patients enrolled that were grouped into pre-and post-CR cohorts and pre- and post-EOS cohorts based on discharge date and concerning implementation of both the UCSD CR program and EOS. The UCSD CR EOS was created to facilitate CR referrals by automatically prompting physicians to enroll eligible patients before hospital discharge. Before the UCSD EOS system, there was no automatic electronic tool to assist physicians in referring patients to CR. The goal of this study was to establish the direct effect that the interventions had on the investigated outcomes. Therefore, 360 patients were recruited close to the launch dates of the UCSD CR program and EOS. The period investigated took into account when the UCSD CR program was the sole CR referral site before the creation of other CR programs that would have confounded the data.
Figure 1: Method flow sheet of enrolling patients, administering survey #1 at week 1, survey #2 at week 6, survey #3 at week 12 of the study, and concluding patient follow-up.
Outcomes
Primary outcomes investigated included referral and participation in CR at different time intervals, week-1 and week-12. Secondary outcomes included the effect of gender, age, race, ethnicity, geography, and subspecialty of referring physicians on CR referral and participation rates.
Geographical stratification
The 2013 National Center for Health Statistics (NCHS) Urban-Rural Classification Scheme for Counties [10] was utilized to stratify patients by geographical locations using home zip codes. Classes included large central metro (counties with a population of 1 million or more), large fringe metro (counties of 1 million or more that do not qualify as large central metro), medium metro (counties of 250,000-999,999), and small metro (counties of < 250,000).
Statistical analysis
Baseline characteristics of the Pre- and post-patient cohorts were expressed as mean with standard deviation and count with percentage and were compared by paired t-tests and chi-square analysis for continuous and categorical variables, respectively. The univariable and multivariable logistic regression model was utilized to assess the impact of establishing a CR program and the availability of an EOS on referral and participation at week-1 and week-12. For multivariable logistic regression, potential confounders such as gender, age, race, ethnicity, geography, subspecialty of referring physician, and insurance were adjusted for in the model.
Patient characteristics of CR and EOS cohort
A total of 360 patients with CHD were enrolled in the study with one patient lost to follow up. The Pre-CR cohort included a total of 184 patients of whom 69.6% were male, with a mean age of 63.6 years, and a racial composition of 58.7% white. The post-CR cohort included 175 patients of whom 76.6% were male, with a mean age of 63.2 years and a racial composition of 48.9% white. The Pre-EOS cohort consisted of 239 patients of whom 71.1% were male, with a mean age of 63.3 years and a racial composition of 57.3% white; while the Post-EOS cohort consisted of 120 patients of whom 76.7% were male, with a mean age of 63.8 years and a racial composition of 47.1% white. Regarding ethnic background, Hispanics comprised 39.1% and 49.4% in the Pre-CR and Post-CR cohorts respectively. Similarly, Hispanics comprised 40.2% and 52.1% in the Pre-EOS and Post-EOS cohorts respectively. See Table 1 for additional details regarding demographic representation.
Table 1 shows Pre-and Post-CR and EOS cohort characteristics.
Table 2 shows medical comorbidities found in the Pre- and Post-CR and EOS cohorts.
Table 3 shows CR referral and participation % in Pre-CR and Post-CR cohorts in weeks 1 and 12.
Table 4 shows CR referral and participation % in Pre-EOS and Post-EOS cohorts in weeks 1 and 12.
| Table 1: Demographic characteristics of patients in the following cohorts (Pre-CR, Post-CR, Pre-EOS, and Post-EOS. | ||||||
| Variable | Pre-CR | Post-CR | p - value | Pre-EOS | Post-EOS | p - value * |
| N = 184 | N = 175 | N = 240 | N = 120 | |||
| Sex | ||||||
| Female | 30.4% | 23.4% | 0.169 | 28.9% | 23.3% | 0.323 |
| Male | 69.6% | 76.6% | 71.1% | 76.7% | ||
| Age | 63.6 | 63.2 | 0.742 | 63.3 | 63.8 | 0.643 |
| Race | ||||||
| Non-white | 41.3% | 51.1% | 0.078 | 42.7% | 52.9% | 0.085 |
| White | 58.7% | 48.9% | 57.3% | 47.1% | ||
| Ethnicity | ||||||
| Hispanic | 39.1% | 49.4% | 0.064 | 40.2% | 52.1% | 0.042 |
| Language | ||||||
| English | 71.7% | 68.0% | 0.511 | 72.0% | 65.8% | 0.283 |
| Non-English | 28.3% | 32.0% | 28.0% | 34.2% | ||
| Language Read | ||||||
| English | 69.6% | 65.5% | 0.099 | 69.9% | 63.0% | 0.165 |
| Mandarin/Cantonese | 0.5% | 0.0% | 0.4% | 0.0% | ||
| Other | 2.2% | 0.0% | 1.7% | 0.0% | ||
| Spanish | 27.7% | 34.5% | 28.0% | 37.0% | ||
| Language Spoken | ||||||
| English | 69.0% | 61.5% | 0.244 | 69.0% | 58.0% | 0.082 |
| Mandarin/Cantonese | 0.5% | 0.0% | 0.4% | 0.0% | ||
| Spanish | 28.3% | 35.6% | 28.9% | 37.8% | ||
| Tagalog or Ilocano | 0.0% | 1.1% | 0.0% | 1.7% | ||
| Other | 2.2% | 1.7% | 1.7% | 2.5% | ||
| City | ||||||
| Rural | 27.7% | 27.0% | 0.975 | 26.8% | 28.6% | 0.816 |
| Urban | 72.3% | 73.0% | 73.2% | 71.4% | ||
| Metro | ||||||
| Large metro | 60.4% | 53.8% | 0.057 | 59.5% | 52.5% | 0.330 |
| Medium metro | 0.5% | 4.0% | 1.7% | 3.4% | ||
| Small metro | 39.0% | 42.2% | 38.8% | 44.1% | ||
| Annual Income | ||||||
| < 15k/yr | 23.4% | 17.8% | 0.282 | 23.0% | 16.0% | 0.103 |
| > 60k/yr | 27.7% | 29.3% | 27.6% | 30.3% | ||
| 0-45k/yr | 10.3% | 6.90% | 8.8% | 8.4% | ||
| 15-30k/yr | 13.6% | 10.9% | 14.6% | 7.6% | ||
| 45-60k/yr | 4.30% | 6.90% | 5.0% | 6.7% | ||
| No disclosure | 20.7% | 28.2% | 20.9% | 31.1% | ||
| Insurance Coverage | ||||||
| HMO | 12.0% | 16.6% | < 0.001*** | 13.8% | 15.0% | < 0.001*** |
| Medical/Medicaid | 22.3% | 22.9% | 22.2% | 23.3% | ||
| Medicare | 11.4% | 29.1% | 13.0% | 34.2% | ||
| Medicare-Medical | 17.9% | 4.0% | 16.3% | 0.8% | ||
| Other | 1.6% | 5.7% | 1.7% | 7.5% | ||
| PPO | 15.2% | 15.4% | 13.8% | 18.3% | ||
| PPO+Medicare | 19.6% | 6.3% | 19.2% | 0.8% | ||
| *p < 0.05 considered statistically significant. | ||||||
| Table 2: Comorbidities of individual cohorts. | ||||||
| Variable | Pre-CR N = 184 |
Post-CR N = 175 |
p - value | Pre-EOS N = 240 |
Post-EOS N = 120 |
p - value |
| Prior CAD | 51.1% | 36.6% | 0.008* | 46.0% | 40.0% | 0.331 |
| CABG | 7.1% | 5.1% | 0.590 | 7.5% | 3.3% | 0.183 |
| DES | 31.5% | 21.1% | 0.035* | 28.0% | 23.3% | 0.409 |
| Smoker | ||||||
| Prior | 74.5% | 73.7% | 0.909 | 75.3% | 71.7% | 0.564 |
| Current | 40.8% | 42.9% | 41.8% | 41.7% | ||
| DM | 45.1% | 34.9% | 0.061 | 42.3% | 35.8% | 0.290 |
| CHF | 6.0% | 6.3% | 1.000 | 5.9% | 6.7% | 0.946 |
| Liver Disease | 2.7% | 4.0% | 0.702 | 3.3% | 3.3% | 1.000 |
| HTN | 82.1% | 76.0% | 0.199 | 79.9% | 87.5% | 0.694 |
| Kidney Disease | 12.0% | 12.6% | 0.987 | 13.4% | 10.0% | 0.451 |
| PAD | 3.3% | 5.1% | 0.531 | 3.8% | 5.0% | 0.786 |
| Atrial Fibrillation | 7.6% | 6.9% | 0.943 | 6.3% | 9.2% | 0.435 |
| CVA | 6.0% | 6.9% | 0.023* | 6.3% | 6.7% | 0.577 |
| Dyslipidemia | 77.7% | 66.0% | < 0.001* | 72.0% | 57.5% | 0.008* |
| *p < 0.05 considered statistically significant. | ||||||
| Table 3: CR Referral and Participation Rates based on Pre-CR and Post-CR Cohorts. | ||||
| CR Referrals | CR Participation | |||
| Week 1 | Week 12 | Week 1 | Week 12 | |
| Pre-CR | 38.6% | 54.1% | 9.9% | 39.4% |
| Post-CR | 54.9% | 59.8% | 7.4% | 21.8% |
| p - value* | 0.003 | 0.386 | 0.773 | 0.020 |
| *p < 0.05 considered statistically significant. | ||||
| Table 4: EOS Cohorts- CR Referral and Participation Rates based on EOS Cohorts. | ||||
| CR Referrals | CR Participation | |||
| Week 1 | Week 12 | Week 1 | Week 12 | |
| Pre-EOS | 40.3% | 54.9% | 7.30% | 36.0% |
| Post-EOS | 58.7% | 60.4% | 10.0% | 20.7% |
| P-value* | 0.001 | 0.394 | 0.736 | 0.038 |
| *p <0.05 considered statistically significant. | ||||
Effect of new CR center on referral and participation rates
The availability of a local CR program in the health system prompted referral rate increases notably at both week-1 (38.6% in Pre-CR versus 54.9% Post-CR, p = 0.003) and week-12 (54.1% Pre-CR versus 59.8% in Post-CR, p = 0.386). Univariate logistic regression analysis revealed patients were more likely to be referred in the Post-CR period; week-1 odd ratio (OR) of 1.93 (95% CI 1.27-2.95) and week-12 OR of 1.26 (95% CI 0.79-2.00). Regardless of referral at week-1 versus week-12 from hospital discharge, both periods showed evidence of increased referrals. Despite such noted increased referral rates, overall participation rates in the post-CR period did not improve compared to pre-CR rates at week 1 (Pre-CR 9.9% and Post-CR 7.4%, p = 0.773) or at week 12 (Pre-CR 39.4% and Post-CR 21.9%, p = 0.020).
Multivariable analysis of referral and participation data revealed non-Hispanic patients were more likely to be referred to CR than Hispanics at both week 1 with OR of 2.89 (95% CI: 1.42-6.04) and week 12 with OR of 3.30 (95% CI: 1.54-7.36). Similarly, geographic location affected CR referral rates, with those patients living in large metropolitan areas being more likely to be referred at week 12 with an OR of 2.00 (95% CI: 1.07-3.78). Lastly, our results revealed cardiothoracic surgeons (OR: 0.46, 95% CI 0.24-0.86) and interventional cardiologists (OR: 0.54, 95% CI: 0.32-0.92) were less likely to refer patients to CR at week 1.
Effect of EOS on CR referral and participation rates
The effects of implementing an electronic ordering system were evident in that Post EOS referral rates increased at week-1 (Pre-EOS 40.3% and Post-EOS 58.7%, p < 0.001) and week-12 (Pre-EOS 54.9% and Post-EOS 60.4%, p = 0.394) with univariate logistic analysis showing patients were more likely to be referred at both week-1 (OR: 2.1, 95% CI 1.4-3.3) and week-12 (OR: 1.25, 95% CI 0.80-1.98). A similar pattern was noted in the multivariable regression analysis when adjusting for confounding factors at both week 1 (OR: 2.2, 95% CI 1.4-3.7) and week 12 (OR: 1.49, 95% CI 0.88-2.53). Ultimately, Post EOS referrals at week 1 and week 12 increased at both time points, indicating the effectiveness of the automatic EOS as a tool.
Furthermore, the multivariable analysis revealed that non-Hispanic patients were approximately 3 times more likely to be referred to CR than Hispanics at both week 1 (OR: 2.96, 95% CI: 1.46-6.19) and week 12 (OR: 3.22, 95% CI: 1.51-7.12). Similarly, patients in large metropolitan areas were noted to be more likely to be referred by week 12 (OR: 2.12, 95% CI: 1.13-4.02). Lastly, cardiothoracic surgeons (OR: 0.453, 95% CI 0.240-0.842) and interventional cardiologists (OR: 0.519, 95% CI: 0.305-0.877) were less likely to refer patients to CR at week 1. A similar trend in referral rates was noted at week 12 for both specialties although such trends did not reach statistical significance at that time interval; interventional cardiology with OR of 0.647 (p = 0.142) and cardiothoracic surgery with OR of 0.547 (p = 0.086).
Regarding CR participation, univariate analysis revealed patients with CHD were more likely to participate at both week 1 (OR: 2.1, 95% CI 1.4-3.3) and week 12 (OR: 1.252, 95% CI 0.80-1.96) following the EOS implementation. Notable findings on the multivariable analysis revealed that non-Hispanics were more likely to participate at both week-1 (OR: 2.96, 95% CI 1.46-6.19) and week 12 (OR: 3.22, 95% CI 1.51-7.12) compared to Hispanics and that patients from large metropolitan areas were more likely to participate by week-12 (OR: 2.124, 95% CI 1.131-4.020).
Effect of local CR center
To our knowledge, this is the first prospective cohort study evaluating the independent impact of the availability of a new CR program and the implementation of an automated electronic ordering system (EOS) on CR referral and participation rates. Valencia, et al. [11] previously characterized the benefits of CR in decreasing cardiac mortality by approximately 25% over 3 years of follow-up and a 50% decrease in recurrent events 6 months following the acute coronary event. Yet, the direct impact of a new CR program with EOS on referral and participation rates has not been fully investigated. In our adjusted analysis comparing the Pre- and Post-CR cohorts, the availability of a local CR program led to an increase in referral rates noted at both week 1 and week 12 in Post-CR; however, such increases in referral rates did not translate into direct enrollment as the overall participation rates decreased in the Post-CR compared to Pre-CR periods. Extraneous factors that may have affected participation include among others, geographical, financial, medical, physical, and personal (Figure 2). Patients’ self-reported factors including geographic barriers (42%), financial costs (20%), personal issues (18%), other reasons (13%), and medical limitations (7%), all negatively impacted CR participation among our patient population. Geographic barriers were the highest self-reported factor partly because many of the patients that are served by UCSD travel from Imperial County, a rural area bordered by Mexico and Arizona, nearly two hours away. The long drive limits in-person participation for a majority of patients. Insurance coverage also affects enrollment and the number of sessions. Many patients are referred but are not aware of the profound, life-changing significance of participating in the holistic CR sessions, and as a result, do not attend. The surveys performed unveiled the medical, personal, geographic, and financial roadblocks to patients, which allows awareness and opportunities to circumvent these current barriers
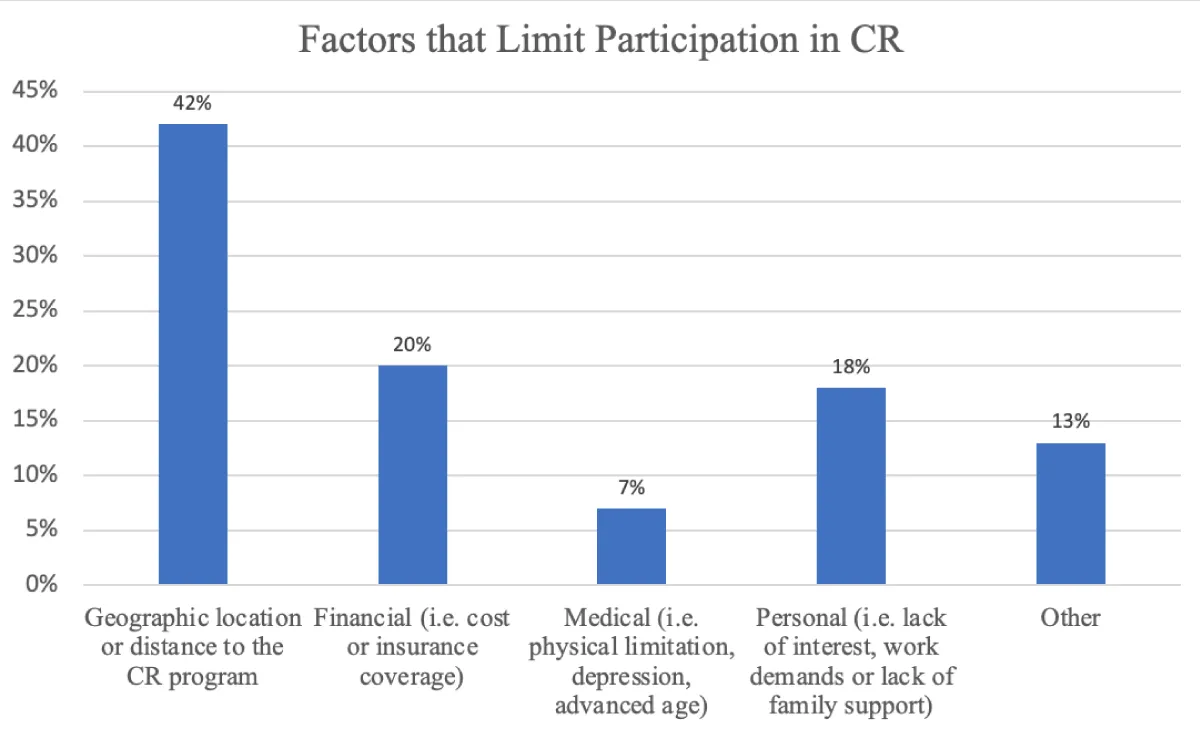
Figure 2: Patients’ self-reported barriers in participation in CR.
Effect of EOS implementation
Referral rate improvements were noted both at week 1 (Pre 40.3% and Post 58.7%, p < 0.001) and week 12 (Pre 54.9% and Post 60.4%, p = 0.394) and were congruent to those published by Grace, et al. [8]. In such a study 661 patients with ACS were followed with and without an automatic referral system in place and found that the implementation of an EOS led to significantly higher referral rates; 67% compared to 34% using the non-electronic referral method. However, the association between EOS implementation and participation rate has not been reported in the literature. Our analysis showed that at week 1, patients were more likely to participate in CR in Post- vs. Pre-EOS. Yet, at week 12, there was a decline in the CR participation rate. It remains unclear as to the specific factors contributing to such a decline in participation rates but we suspect cost, distance to the CR center, and even loss of interest may be significant factors contributing to these findings as shown in Figure 2.
Disparities in referring physicians, ethnicity, geography
CR is an effective therapy for the treatment of CHD and yet there is underutilization amongst racial and ethnic minorities [12-14]. Research has shown that racial and ethnic groups with CHD are less likely to participate in CR compared to white patients; factors such as annual earned income, rural predominance of non-white patients, and language barriers contribute to this divide [15]. Racial and Ethnic minority status predicts lower referral rates to CR; The American Heart Association showed that 39% of Hispanics are referred by their physicians compared to 56% and 58% of Black and white populations respectively [16]. A similar pattern emerged in an analysis of 601,000 Medicare patients which showed greater participation rates among whites vs. non-whites after myocardial infarction or coronary artery bypass graft surgery [17]. Additionally, it has been noted healthcare providers also play a key role in propagating disparities in medical treatment of cardiac rehabilitation by being the ones in control of referrals [13,17].
This study found similar disparities in referral and participation disparities within the population evaluated. On both CR and EOS cohorts, White patients were more likely to be referred and participate in CR than Hispanics at week 1 and week 12. Concordant with past research [11,18], geographical location impacted referral and participation rates as we noted that by week 12 in our EOS cohort, patients from urban areas were more likely to be referred to CR than patients from rural areas. Lastly, in both the CR and EOS cohorts, at week 1, general cardiologists were twice more likely to refer patients to CR than cardiothoracic surgeons (p =0.013) and interventional cardiologists (p = 0.015). These results show how even physician specialty can impact CR referral likelihood.
Clinical and policy implications
Patients with CHD benefit from a CR program that encompasses physical and mental health and wellness, but CR referral and participation are surprisingly low. Our results suggest that the implementation of a local CR program and EOS are associated with improved CR referral rates. Further studies are needed to focus on improving CR enrollment and participation and understanding the barriers to low enrollment rates after initial referral. We proposed further evaluation of EOS on CR referral rates among racial and ethnic minority groups as well as populations living in rural settings.
Given the relatively low percentage of patients with CHD who participate in supervised hospital-based CR, alternative approaches to provide CR have been recommended by cardiovascular societies [19-21]. The convenience of a home-based CR program may increase participation rates in patients who have limited access to traditional CR programs [21]. Several CR models of delivery services that include home-based programs, internet-based modules, and community-based group programs with guidance by nurses and health professionals, provide alternative paradigms that may increase patient participation in CR [13]. Specifically, home-based programs appear to provide an excellent alternative to patients with geographical, financial, and social limitations such as those served at our institution without compromising the proven benefits of CR [20,21].
Study limitations
Our analysis was limited by a sample size of 360 patients from four quaternary hospitals in Southern California, which limits the statistical power of the study and analysis. Additionally, the study was not blinded and this could have influenced CR referral patterns by physicians. It is plausible that CR enrollment and participation might have been affected by insurance coverage which we recognize to be an important as well as a possible confounding factor in our study. Future studies should include insurance status to assess the impact of this important variable on CR referral, enrollment, and participation rates. This study is vulnerable to secular trends, given it is a pre-post study.
This prospective study investigated the effects of implementing a local cardiac rehabilitation program and an electronic ordering system for patients hospitalized with CHD. Our analysis revealed increased CR referral rates at week 1 and week 12 with the long-term potential of increasing referral rates amongst patients with CHD. Factors such as the patient’s ethnic background, home geography, and specialty of the referring physician appear to be significant contributors to low referral and participation rates. Local CR programs and the implementation of EOS may extend the positive impact of CR for patients with CHD as well as ameliorate underlying cardiovascular health disparities that affect racial and ethnic groups.
Ethical declarations
Patient consent was obtained and IRB 170551 for UCSD Trial: Observational Study to Evaluate Cardiac Rehabilitation Referral and Participation Rates of Vulnerable Groups with Coronary Heart Disease.
Sources of funding
Hispanic Center of Excellence Scholars Scholarship for Research Grant and Award, 2019.
- Balady GJ, Williams MA, Ades PA, Bittner V, Comoss P, Foody JA, Franklin B, Sanderson B, Southard D; American Heart Association Exercise, Cardiac Rehabilitation, and Prevention Committee; Council on Clinical Cardiology; Councils on Cardiovascular Nursing, Epidemiology and Prevention, and Nutrition, Physical Activity, and Metabolism; American Association of Cardiovascular and Pulmonary Rehabilitation. Core components of cardiac rehabilitation/secondary prevention programs: 2007 update: a scientific statement from the American Heart Association Exercise, Cardiac Rehabilitation, and Prevention Committee, the Council on Clinical Cardiology; the Councils on Cardiovascular Nursing, Epidemiology and Prevention, and Nutrition, Physical Activity, and Metabolism; and the American Association of Cardiovascular and Pulmonary Rehabilitation. J Cardiopulm Rehabil Prev. 2007 May-Jun;27(3):121-9. doi: 10.1097/01.HCR.0000270696.01635.aa. PMID: 17558191.
- Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, DePalma SM, Gidding S, Jamerson KA, Jones DW, MacLaughlin EJ, Muntner P, Ovbiagele B, Smith SC Jr, Spencer CC, Stafford RS, Taler SJ, Thomas RJ, Williams KA Sr, Williamson JD, Wright JT Jr. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension. 2018 Jun;71(6):1269-1324. doi: 10.1161/HYP.0000000000000066. Epub 2017 Nov 13. Erratum in: Hypertension. 2018 Jun;71(6):e136-e139. doi: 10.1161/HYP.0000000000000075. Erratum in: Hypertension. 2018 Sep;72(3):e33. doi: 10.1161/HYP.0000000000000080. PMID: 29133354.
- Thomas RJ, King M, Lui K, Oldridge N, Piña IL, Spertus J; ACCFAHA Task Force on Performance Measures. AACVPR/ACCF/AHA 2010 Update: Performance measures on cardiac rehabilitation for referral to cardiac rehabilitation/secondary prevention services: A report of the American Association of Cardiovascular and Pulmonary Rehabilitation and the American College of Cardiology Foundation/American Heart Association Task Force on Performance Measures (Writing Committee to Develop Clinical Performance Measures for Cardiac Rehabilitation). J Cardiopulm Rehabil Prev. 2010 Sep-Oct;30(5):279-88. doi: 10.1097/HCR.0b013e3181f5e36f. PMID: 20808157.
- Smith SC Jr, Benjamin EJ, Bonow RO, Braun LT, Creager MA, Franklin BA, Gibbons RJ, Grundy SM, Hiratzka LF, Jones DW, Lloyd-Jones DM, Minissian M, Mosca L, Peterson ED, Sacco RL, Spertus J, Stein JH, Taubert KA. AHA/ACCF secondary prevention and risk reduction therapy for patients with coronary and other atherosclerotic vascular disease: 2011 update: a guideline from the American Heart Association and American College of Cardiology Foundation endorsed by the World Heart Federation and the Preventive Cardiovascular Nurses Association. J Am Coll Cardiol. 2011 Nov 29;58(23):2432-46. doi: 10.1016/j.jacc.2011.10.824. Epub 2011 Nov 3. Erratum in: J Am Coll Cardiol. 2015 Apr 14;65(14):1495. Dosage error in article text. PMID: 22055990.
- Suaya JA, Shepard DS, Normand SL, Ades PA, Prottas J, Stason WB. Use of cardiac rehabilitation by Medicare beneficiaries after myocardial infarction or coronary bypass surgery. Circulation. 2007 Oct 9;116(15):1653-62. doi: 10.1161/CIRCULATIONAHA.107.701466. Epub 2007 Sep 24. PMID: 17893274.
- Ades PA, Keteyian SJ, Wright JS, Hamm LF, Lui K, Newlin K, Shepard DS, Thomas RJ. Increasing Cardiac Rehabilitation Participation From 20% to 70%: A Road Map From the Million Hearts Cardiac Rehabilitation Collaborative. Mayo Clin Proc. 2017 Feb;92(2):234-242. doi: 10.1016/j.mayocp.2016.10.014. Epub 2016 Nov 15. PMID: 27855953; PMCID: PMC5292280.
- American Heart Association. Get With The Guidelines. 2009. http://www.americanheart.org/presenter.jhtml?identifier=1165
- Grace SL, Scholey P, Suskin N, Arthur HM, Brooks D, Jaglal S, Abramson BL, Stewart DE. A prospective comparison of cardiac rehabilitation enrollment following automatic vs usual referral. J Rehabil Med. 2007 Apr;39(3):239-45. doi: 10.2340/16501977-0046. PMID: 17468793; PMCID: PMC2935486.
- LaBresh KA, Ellrodt AG, Gliklich R, Liljestrand J, Peto R. Get with the guidelines for cardiovascular secondary prevention: pilot results. Arch Intern Med. 2004 Jan 26;164(2):203-9. doi: 10.1001/archinte.164.2.203. PMID: 14744845.
- Ingram DD, Franco SJ. 2013 NCHS Urban-Rural Classification Scheme for Counties. Vital Health Stat 2. 2014 Apr;(166):1-73. PMID: 24776070.
- Valencia HE, Savage PD, Ades PA. Cardiac rehabilitation participation in underserved populations. Minorities, low socioeconomic, and rural residents. J Cardiopulm Rehabil Prev. 2011 Jul-Aug;31(4):203-10. doi: 10.1097/HCR.0b013e318220a7da. PMID: 21705915.
- Castellanos LR, Viramontes O, Bains NK, Zepeda IA. Disparities in Cardiac Rehabilitation among Individuals from Racial and Ethnic Groups and Rural Communities-A Systematic Review. J Racial Ethn Health Disparities. 2019 Feb; 6(1):1-11. doi: 10.1007/s40615-018-0478-x. Epub 2018 Mar 13. PMID: 29536369.
- Chindhy S, Taub PR, Lavie CJ, Shen J. Current challenges in cardiac rehabilitation: strategies to overcome social factors and attendance barriers. Expert Rev Cardiovasc Ther. 2020 Nov; 18(11):777-789. doi: 10.1080/14779072.2020.1816464. Epub 2020 Sep 14. PMID: 32885702; PMCID: PMC7749053.
- Ritchey MD, Maresh S, McNeely J, Shaffer T, Jackson SL, Keteyian SJ, Brawner CA, Whooley MA, Chang T, Stolp H, Schieb L, Wright J. Tracking Cardiac Rehabilitation Participation and Completion Among Medicare Beneficiaries to Inform the Efforts of a National Initiative. Circ Cardiovasc Qual Outcomes. 2020 Jan;13(1):e005902. doi: 10.1161/CIRCOUTCOMES.119.005902. Epub 2020 Jan 14. PMID: 31931615; PMCID: PMC8091573.
- Dang Y-X, Nunez SR, Gallegos A, Viramontes O, Zepeda I, Castellanos L. Non-White Patients With Coronary Heart Disease Have Worse Cardiac Rehabilitation Participation Than White Patients. J Am Coll Cardiol 2017; 69:1848.
- Brown TM, Hernandez AF, Bittner V, Cannon CP, Ellrodt G, Liang L, Peterson ED, Piña IL, Safford MM, Fonarow GC; American Heart Association Get With The Guidelines Investigators. Predictors of cardiac rehabilitation referral in coronary artery disease patients: findings from the American Heart Association's Get with the Guidelines Program. J Am Coll Cardiol. 2009 Aug 4;54(6):515-21. doi: 10.1016/j.jacc.2009.02.080. PMID: 19643312; PMCID: PMC2760436.
- Thomas RJ, King M, Lui K, Oldridge N, Piña IL, Spertus J; ACC/AHA Task Force Members. AACVPR/ACC/AHA 2007 performance measures on cardiac rehabilitation for referral to and delivery of cardiac rehabilitation/secondary prevention services. J Cardiopulm Rehabil Prev. 2007 Sep-Oct;27(5):260-90. doi: 10.1097/01.HCR.0000291295.24776.7b. PMID: 17885506.
- Shanmugasegaram S, Oh P, Reid RD, McCumber T, Grace SL. Cardiac rehabilitation barriers by rurality and socioeconomic status: a cross-sectional study. Int J Equity Health. 2013 Aug 28;12:72. doi: 10.1186/1475-9276-12-72. PMID: 23985017; PMCID: PMC3765803.
- Wenger NK, Froelicher ES, Smith LK, Ades PA, Berra K, Blumenthal JA, Certo CM, Dattilo AM, Davis D, DeBusk RF, et al. Cardiac rehabilitation as secondary prevention. Agency for Health Care Policy and Research and National Heart, Lung, and Blood Institute. Clin Pract Guidel Quick Ref Guide Clin. 1995 Oct;(17):1-23. PMID: 8595435.
- Snoek JA, Prescott EI, van der Velde AE, Eijsvogels TMH, Mikkelsen N, Prins LF, Bruins W, Meindersma E, González-Juanatey JR, Peña-Gil C, González-Salvado V, Moatemri F, Iliou MC, Marcin T, Eser P, Wilhelm M, Van't Hof AWJ, de Kluiver EP. Effectiveness of Home-Based Mobile Guided Cardiac Rehabilitation as Alternative Strategy for Nonparticipation in Clinic-Based Cardiac Rehabilitation Among Elderly Patients in Europe: A Randomized Clinical Trial. JAMA Cardiol. 2021 Apr 1;6(4):463-468. doi: 10.1001/jamacardio.2020.5218. PMID: 33112363; PMCID: PMC7593879.
- Thomas RJ, Beatty AL, Beckie TM, Brewer LC, Brown TM, Forman DE, Franklin BA, Keteyian SJ, Kitzman DW, Regensteiner JG, Sanderson BK, Whooley MA. Home-Based Cardiac Rehabilitation: A Scientific Statement from the American Association of Cardiovascular and Pulmonary Rehabilitation, the American Heart Association, and the American College of Cardiology. Circulation. 2019 Jul 2;140(1):e69-e89. doi: 10.1161/CIR.0000000000000663. Epub 2019 May 13. PMID: 31082266.