
More Information
Submitted: 22 January 2020 | Approved: 17 February 2020 | Published: 18 February 2020
How to cite this article: Rafla S, Kamal A. ECG interpretation and commentary. J Cardiol Cardiovasc Med. 2020; 5: 034-041.
DOI: 10.29328/journal.jccm.1001083
ORCiD: orcid.org/0000-0001-8688-6532
Copyright License: © 2020 Rafla S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Long QT syndrome; Brugada syndrome; Arrhythmogenic RV dysplasia; Supraventricular tachycardia; Ventricular tachycardia
Abbreviations: WPWs: Wolff Parkinson White syndrome; LBB: Left Bundle Block; RBB: Right Bundle Block; AVNRT: Atrioventricular Nodal Reentrant Tachycardia; AVRT: Atrioventricular Reentrant Tachycardia; CRT: Cardiac Resynchronization Therapy

ECG interpretation and commentary
Samir Rafla1*, Ahmed Mokhtar2 and Amr Kamal3
1Emeritus Professor, Cardiology Department, Alexandria University, Egypt
2Lecturer of Cardiology, Faculty of Medicine, Alexandria University, Egypt
3Lecturer of Cardiology, Alexandria University, Egypt
*Address for Correspondence: Samir Rafla, MD, FACC, EFESC, FHRS, Emeritus Professor, Cardiology Department, Alexandria University, Egypt, Tel: 00201001495577; Email: [email protected]
This is demonstration of selected ECGs for learning or for exams; guided by lessons from great teachers as Prof. Hein Wellens MD. Here we provide advanced examples with comment and analysis.
The electrocardiogram is and will continue to be a very important tool for diagnosis of many cardiac disorders [1-7]. It is a simple noninvasive technique. It is not expensive and available everywhere; but the most important is the correct interpretation. We hope the examples given here help and assist under and post graduate doctors in this field.
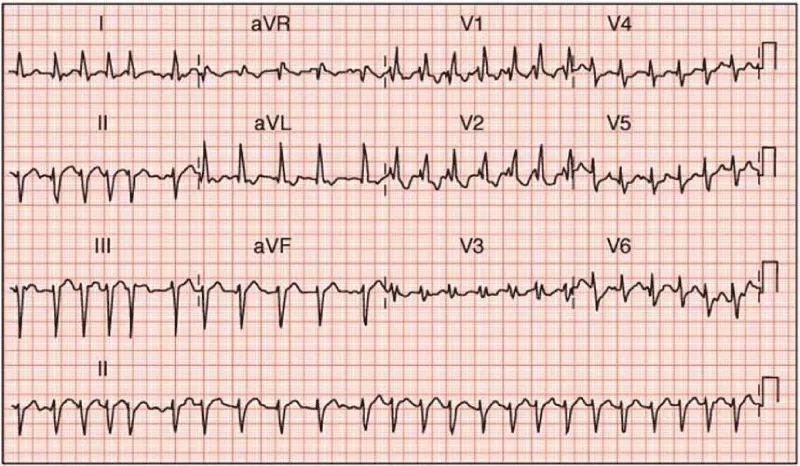
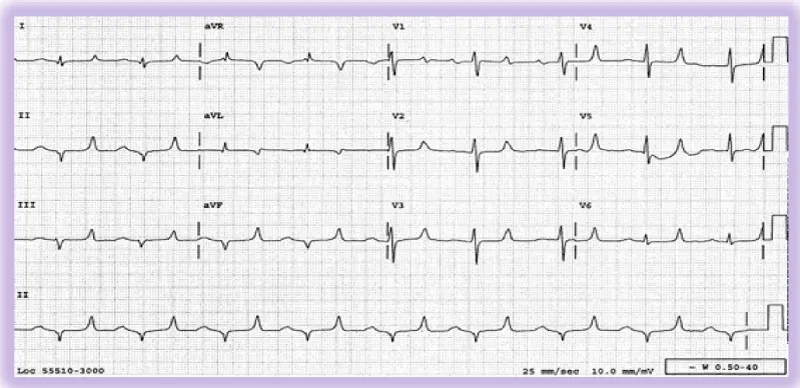
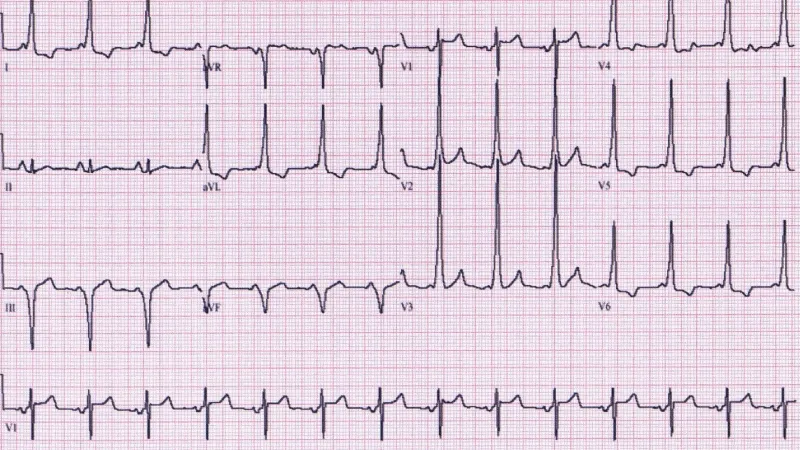
Case 1: Comment: Atrial fibrillation; right bundle block with left axis, left anterior hemiblock so say bifascicular block; ST changes in V4, V5 suggest many possibilities as ischemia or LV hypertrophy, or myocardial disease.
Case 1:
A bifascicular block can occur as a part of the ischemic heart disease or as a part of the normal degeneration of the conduction system (Lev’s disease). Although the 2009 American College of Cardiology/American Heart Association scientific statement on ECG interpretation does not recommend the use of the terms “bifascicular” or “trifascicular,” they are quite commonly used.
Management: Lanoxin digoxin, Amiodarone (Cordarone) for a trial period, check thyroid function plus other necessary lab work. Remember new oral anticoagulants eg. Rivaroxaban (XANOXIBAN) 20 mg with meal. Treat other comorbidities as hypertension, diabetes, obesity, renal insufficiency, electrolyte imbalance, diuretics for heart failure.
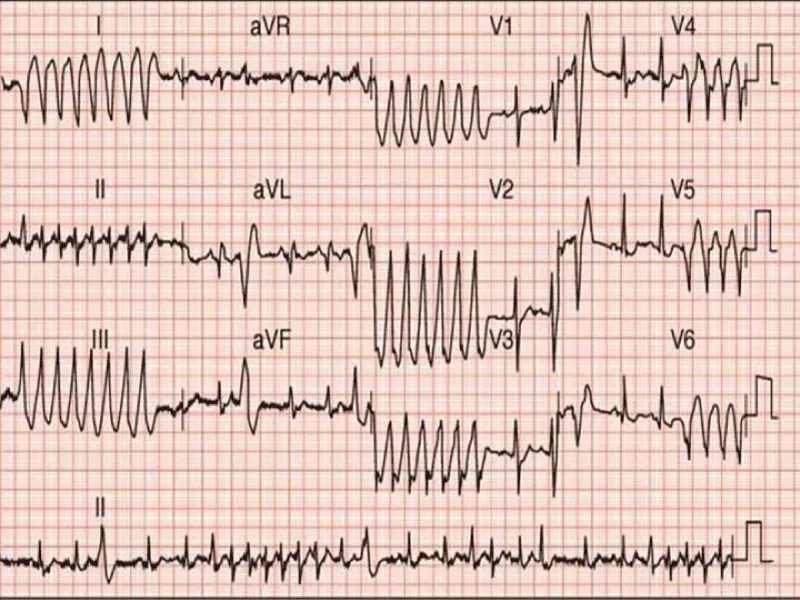
Case 2: None sustained ventricular tachycardia.
Case 2:
Management: First admit patient to intensive care immediately. Give I.V. Xylocaine or Amiodarone two ampoules each 150 mg. Treat any predisposing factors, electrolyte imbalance, Multivessel coronary narrowing, heart failure, thyroid or renal dysfunction. ST depression in V4, 5, 6 suggest ischemia or LV hypertrophy or cardiomyopathy. Remember Entresto (Sacuptril-Valsartan) that improves LV function if ejection fraction is below 40%. I do not see sure evidence of accessory pathway, or atrial fibrillation.
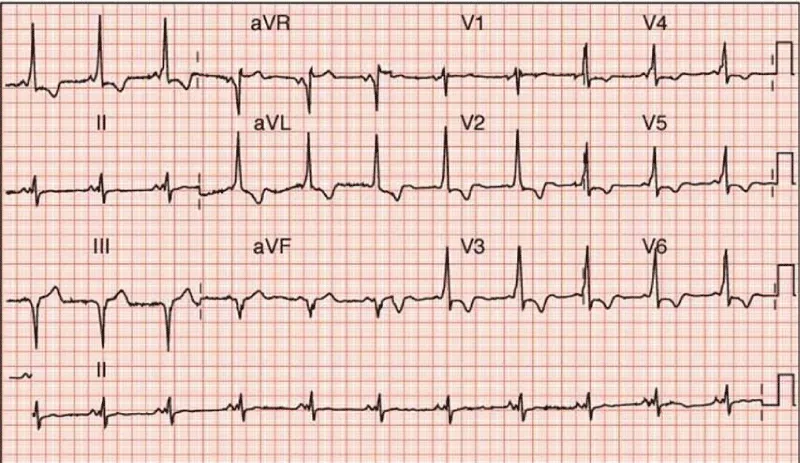
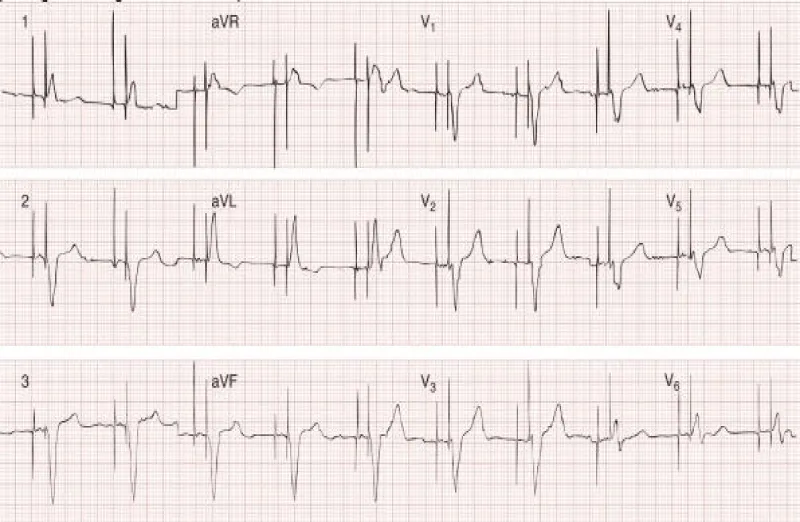
Case 3: Wolff Parkinson White Syndrome (WPWs), Preexcitation syndrome or accessory pathway. Because the delta wave in lead I and aVL is positive and in lead aVR is negative. Right side accessory pathway is preferred, LIII and aVF show Q wave as if inferior infarction so accessory pathway is posteroseptal. Note the short PR and the delta wave in LII, V3, 4, 5, 6. Management is ablation.
Case 3:
The typical ECG finding of WPW is a short PR interval and a “delta wave”. A delta wave is slurring of the upstroke of the QRS complex. This occurs since the action potential from the SA node is able to conduct to the ventricles very fast through the accessory pathway, so the QRS occurs immediately after the P wave making the delta wave.
When WPW occurs in the setting of atrial fibrillation, the fast atrial rate of 400-600 can conduct quite rapidly to the ventricles. If AV nodal blocking drugs such as beta-blockers or non-dihydropyridine calcium channel blockers are given in this setting, the conduction through the accessory pathway will be enhanced. This occurs since the accessory pathway is not subject to block by these medications; however the AV node is resulting in fewer action potentials traveling through the AV node and more through the accessory pathway. Procainamide or emergency cardioversion is the treatment of choice in the setting of WPW and atrial fibrillation.
Ventricular tachycardia
Ventricular tachycardia refers to a heart rhythm originating in the ventricles at a rate of greater than 100 beats per minute. This can be hemodynamically unstable causing severe hypotension and thus is life-threatening. Ventricular fibrillation, asystole and sudden cardiac death can occur soon after ventricular tachycardia if action is not taken immediately.
Sustained ventricular tachycardia VT is defined as lasting greater than 30 seconds or symptomatic. Non-sustained is less than 30 seconds and asymptomatic.
Ventricular tachycardia should be described by type (monomorphic or polymorphic), duration (sustained versus non-sustained) and heart rate. For example, monomorphic VT non-sustained at a heart rate of 220 beats per minute or sustained polymorphic ventricular tachycardia at a heart rate of 250 beats per minute.
Polymorphic ventricular tachycardia (Torsades de Pointes) has multiple QRS morphologies. Polymorphic ventricular tachycardia is best treated with intravenous magnesium. Patients with a prolonged QT interval have a higher risk of developing polymorphic VT. Removing offending drugs that prolong the QT interval and correcting potassium or calcium imbalances are crucial.
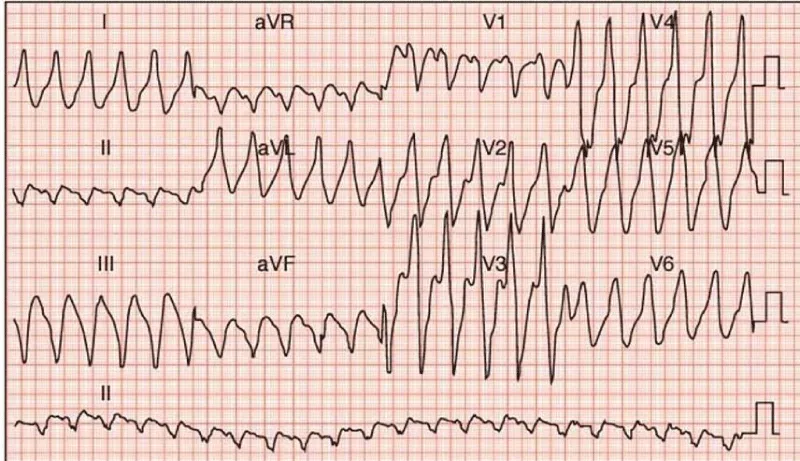
Case 4: Ventricular tachycardia, note AV dissociation evident in LIII and aVF. QRS > 140 msec so sure it is V Tach.
Case 4:
Management: cardioversion. Try IV Xylocaine or two amp amiodarone till DC is ready. Value of amiodarone before DC: 1- it may revert it to sinus rhythm before resorting to electric shock, 2- After success of reversal to sinus rhythm, amiodarone may prevent its recurrence as it is possible. 3- Amiodarone makes DC successful from first shot and at lower joules. Treat predisposing pathologies.
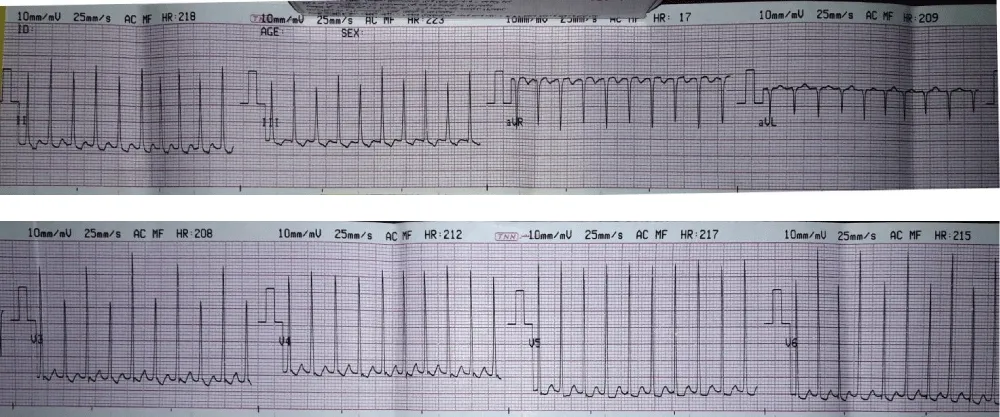
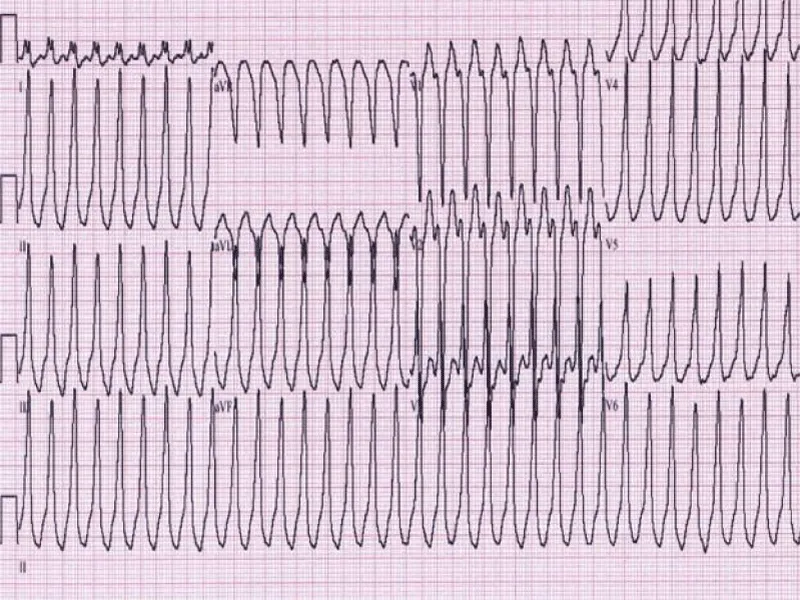
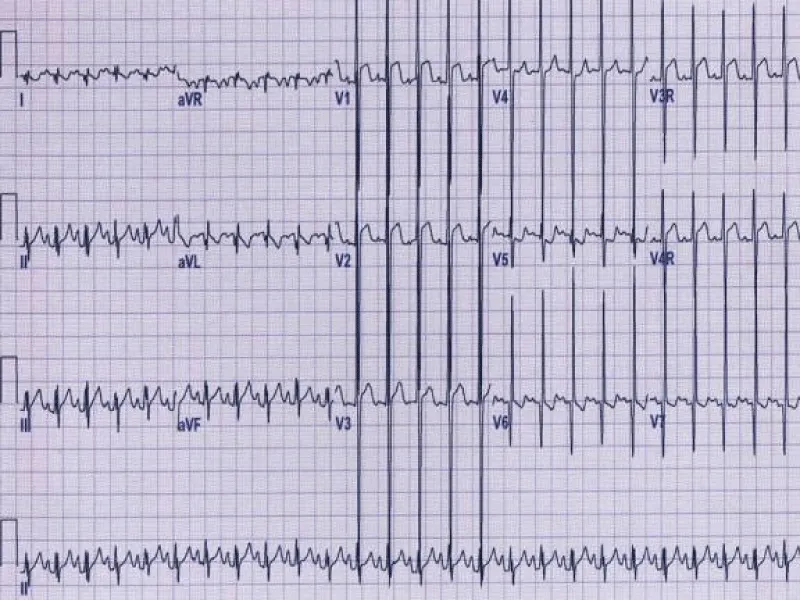
Case 5: Supraventricular tachycardia (accessory pathway) AVRT antidromic AVRT (antegrade conduction through accessory pathway and retrograde through AV node, rate 260 per minute; DC cardioversion is needed immediately.
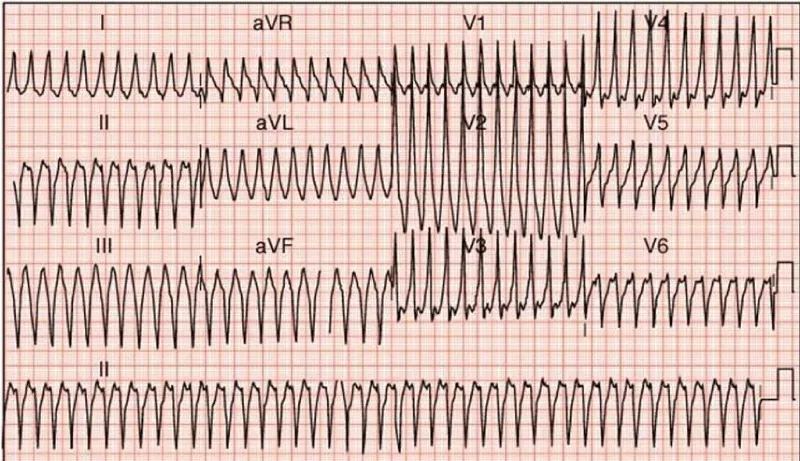
Case 5:
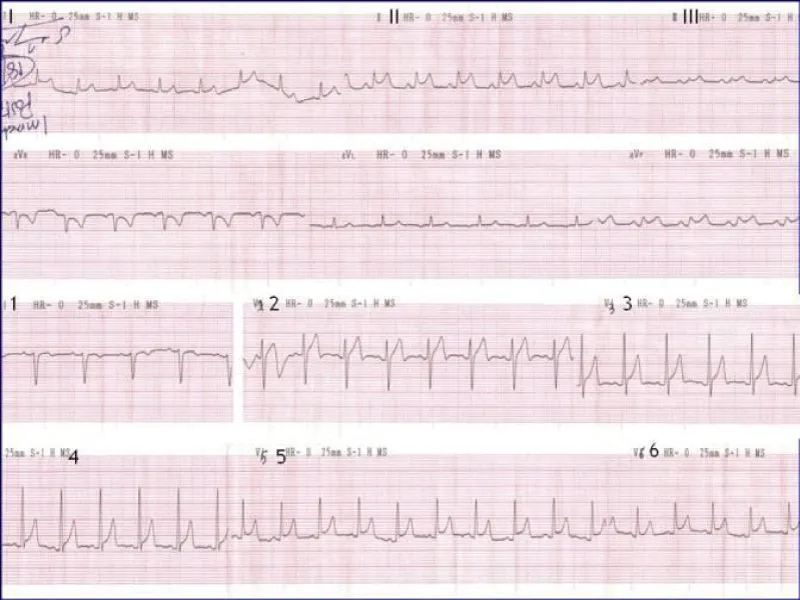
Case 6: Supraventricular tachycardia with aberrant conduction; AV nodal tachycardia (AVRT) involving accessory pathway → Supraventricular tachycardia with aberrant conduction i.e. AV reentry tachycardia (AVRT) involving accessory pathway. V1 shows RBB pattern so it is left sided accessory pathway, aVF does not show Q wave so it is anteroseptal pathway.
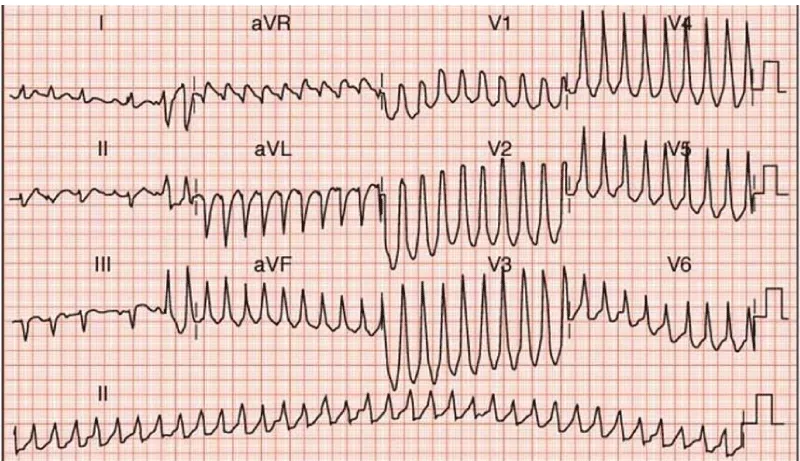
Case 6:
The combination of WPW and atrial fibrillation can potentially be fatal, especially if AV blocking agents are given (remember “ABCD” for adenosine or amiodarone, beta-blockers, calcium channel blockers and digoxin). The medical treatment is procainamide ― though electrical cardioversion is reasonable, especially with hemodynamic instability.
If an AV blocking agent is given, fewer atrial action potentials will pass through the AV node, and more will pass through the accessory pathway. This paradoxically increases the ventricular rate, potentially causing the fatal, hemodynamically unstable rhythm ventricular fibrillation. Procainamide or electrical cardioversion is recommended in these situations (Table 1).
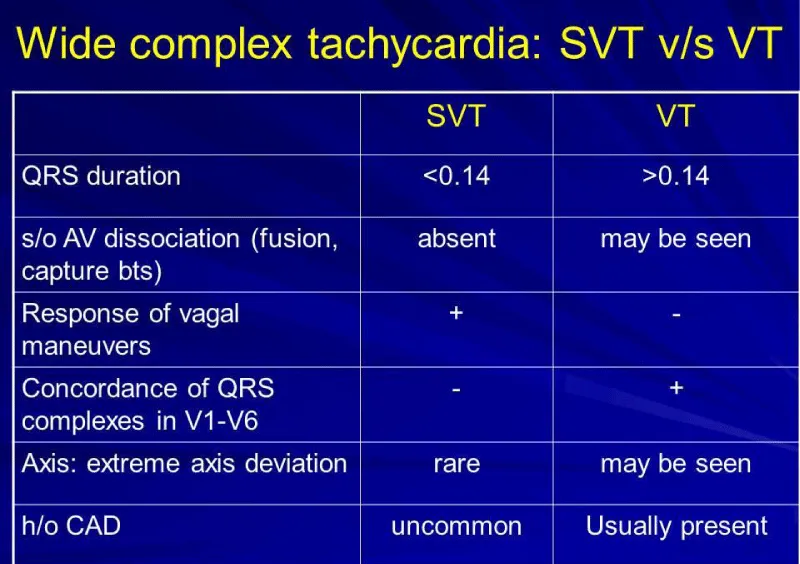
Table 1:
Ventricular tachycardia can be difficult to distinguish from SVT (supraventricular tachycardia) with aberrancy. The Brugada Criteria are most commonly used to distinguish these two entities which are clinically important. Fusion beats and capture beats are also helpful is present to diagnose VT. A few general rules apply to diagnosing ventricular tachycardia (VT):
The Brugada criteria/algorithm is below:
1. Do you see concordance present in the precordial leads (leads V1-V6)?
Also sometime explained as the absence of an RS complex, concordance is diagnostic of VT; are all of the QRS complexes completely upright or completely downward in the precordial leads? If the answer is yes, then VT is the diagnosis.
2. Is the R to S interval > 100 ms in any one precordial lead? If present, then VT is the diagnosis. Simply use calipers to measure the distance between the R wave to S wave in each precordial lead and see if it exceeds 100 ms.
3. Do you see atrioventricular (AV) dissociation? If present, the diagnosis is ventricular tachycardia. AV dissociation occurs when P wave are seen at different rates than the QRS complex.
4. Examine the morphology of the QRS complex to see if it meets the below specific criteria for VT as below.
VT is frequently either in a right bundle branch block pattern (upright in V1) or a left bundle branch block pattern (downward in V1).
If upward in lead V1 (RBBB pattern), then VT is present in the following situations:
- A monophasic R or biphasic qR complex in V1.
- If an RSR’ pattern (“bunny-ear”) is present in V1 with the R peak being higher in amplitude than the R’ peak, then VT is present.
- A rS complex in lead V6 favors VT
If downward in lead V1 (LBBB pattern), then VT is present in the following situations:
- The presence of any Q or QS wave in lead V6 favors VT
- A wide R wave in lead V1 or V2 of 40 ms or more favors VT
- Slurred or notched downstroke of the S wave in V1 or V2 favors VT
- Duration of onset of QRS complex to peak of QS or S wave > 60 mm favors VT
A fusion beat can occur during ventricular tachycardia. The sinus node activity (P wave) can begin to conduct through the normal conduction pathway during an episode of ventricular tachycardia. The abnormal ventricular impulse then conducts retrograde across the AV node and the resulting QRS is a “fusion beat” of the normal QRS morphology and that of the ventricular morphology from the ventricular tachycardia.
A “capture beat” is similar to a fusion beat, except the QRS morphology looks completely like the normal QRS complex since sinus node impulse conducts to the ventricles before the retrograde ventricular activation occurs.
Case 7: Supraventricular tachycardia, AVNRT. P wave not seen, in V1 there is rsr’, the r’ can be the P wave hidden by the ventricular depolarization. Management: DC if uncompensated (pulmonary edema or shock), Adenosine amp 6 mg is first choice, if not successful try two more ampoules adenosine (12 mg), if not available or not successful add Isoptin ampoule 5 mg. If not reverted to sinus rhythm try amiodarone amp one or two IV; other effective drugs propafenone (Rytmonorm), Flecainide. Ablation if attack recurs.
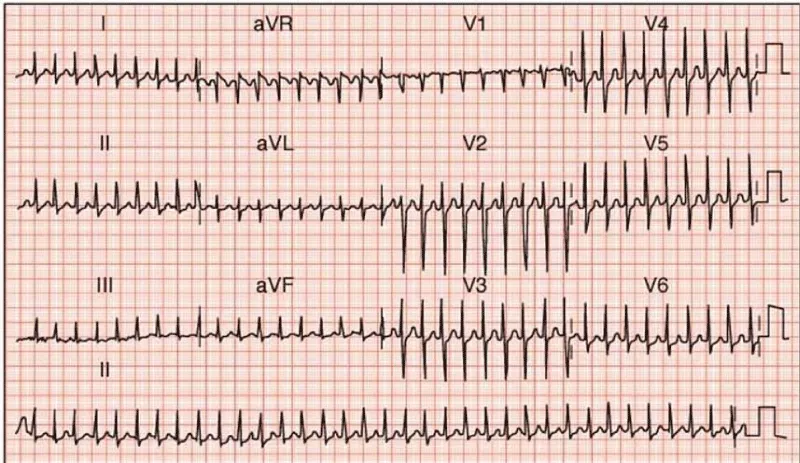
Case 7:
Case 8: Supraventricular tachycardia (AVRT) with electric alternans→Paroxysmal supraventricular tachycardia (PSVT) with electrical alternans.
Can we expect during ablation that there are two accessory pathways or two mechanisms of SVT? As AVRT and also AVNRT.
Case 8:
Long QT syndrome
The normal QTc is 0.44 s. but maybe longer 0.46 for men and 0.47 for women, with a range ± 15% of the mean value. The risk of developing VT is related to the length of the QTc interval. T Wave lumps in the ECG suggest the presence of the long QT syndrome.
To accurately measure the QT interval, multiple leads must be analyzed and longest QT interval is used (since T wave morphology differs from lead to lead). A good way to estimate if the QT interval prolonged is by checking the relation of the QT interval to the R-R interval. If the QT interval terminates before the half-way point between two R waves, then it is not prolonged. If the QT interval terminates after the half-way point between two R waves, then it is prolonged.
The QTc or “corrected QT interval” attempts to determine if the QT interval is prolonged relative to the heart rate (remember bradycardia normally prolongs the QT interval). It is calculated by dividing the measured QT interval by the square root of the R-R interval. The QTc is the most commonly used measurement and not the uncorrected QT interval.
Case 9: Congenital LQT Syndrome: more than 10 genotypes the most common are LQTS1, LQTS2, and LQTS3. Broad based T wave: LQTS1.
Case 9:
Case 10: Congenital LQTS: more than 10 genotypes the most common are LQTS1, LQTS2, and LQTS3. LQTS3 (long isoelectric line preceding the T, biphasic T.
Case 10:
Case 11: Acquired LQTS: eg. Drugs, electrolyte disturbances, hypokalemia.
Case 11:
Case 12: Acquired LQTS: e.g. Drugs, electrolyte disturbances: Hypokalemia.
Case 12:
Case 13: Short QT syndrome: Congenital or acquired. High probability when QTc < 320 ms: Hypercalcemia.
Case 13:
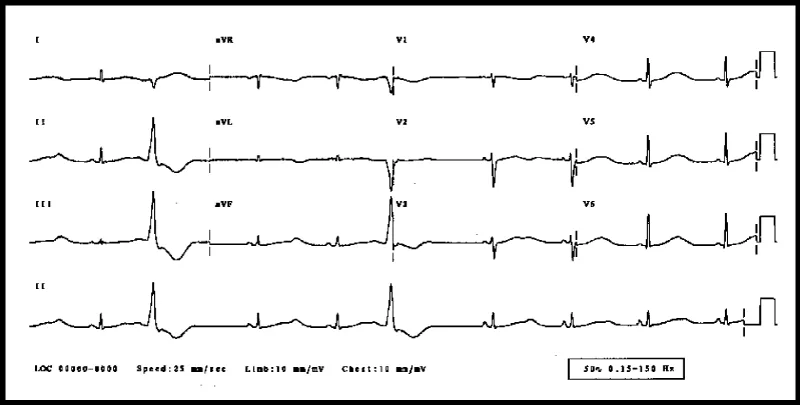
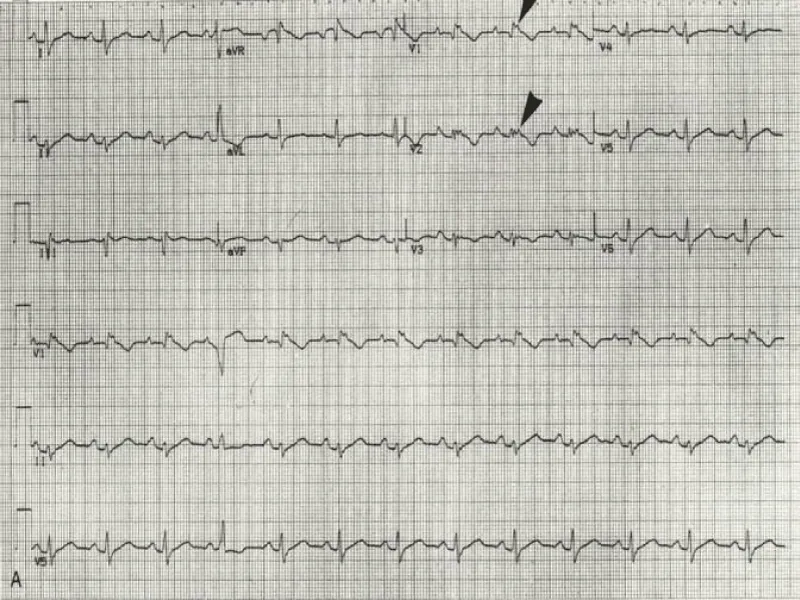
Case 14a: Normal sinus rhythm in a patient with arrhythmogenic right ventricular dysplasia. The arrowheads point to late right ventricular activation called an epsilon wave.
Case 14a:
The classic ECG findings in arrhythmogenic right ventricular dysplasia are inverted T waves in the right precordial leads (V1-V3) with an “epsilon wave” just after the QRS in lead V1, representing early afterdepolarizations or “late potentials.”
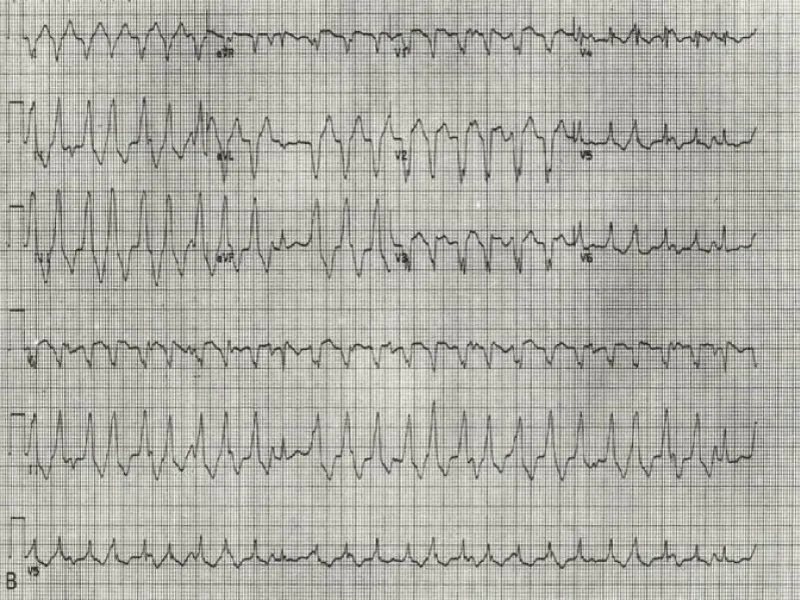
Case 14b: Ventricular tachycardia in the same patient with right ventricular dysplasia.
Case 14b:
Case 15: VT 205/min, LBBB with right axis. Remember right ventricular dysplasia or right ventricular outflow tract tachycardia.
Case 15:
Case 16: This appears to be dual chamber pacing but the QRS is not wide and is not typical LBB as when we pace from RV, so this is cardiac resynchronization pacing (biventricular pacing).
Case 16:
CRT is indicated in patients with LBB and EF < 35%.
Case 17: Pacemaker Malfunction: undersensing.
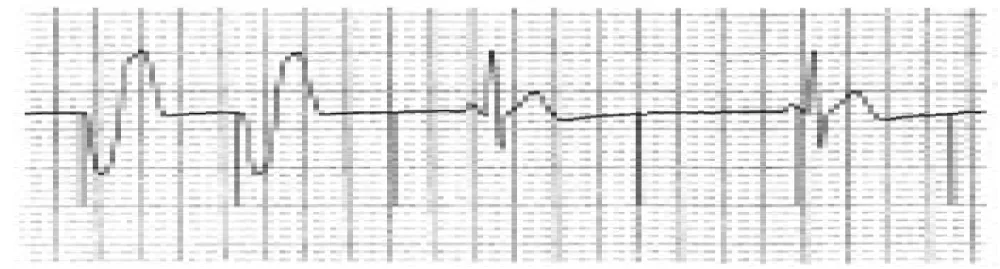
Case 17:
Possible Causes of undersensing (Table 2).
| Table 2: Possible Causes of undersensing. |
| Possible Causes of undersensing Corrective Measures |
| • Threshold rise • Increase output (mA)/check thresholds |
| • Fractured/dislodged lead • Replace/reposition lead |
| • Battery depletion • Replace battery |
| • QRS not visible • Adjust ECG |
| • Tissue is refractory • Assess mode selection |
| • Faulty cable connections • Check connections |
| • Switch polarity (epicardial system |
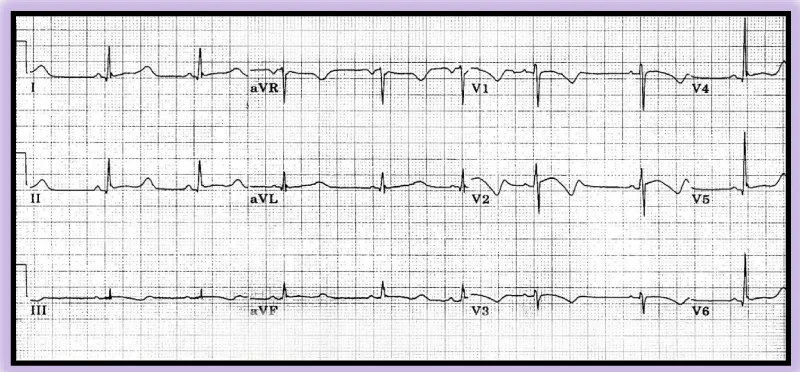
Case 18: Acute pericarditis. Coronary angio revealed single right coronary lesion. Pericardial effusion progressed to constrictive effusive pericarditis.
Case 18:
Note: The ECG changes of pericarditis must be distinguished from those of early repolarization. The ST elevation seen in early repolarization is very similar; diffuse and concave upward. However, three things may help to distinguish pericarditis from early repolarization:
1) The ratio of the T wave amplitude to the ST elevation should be > 4 if early repolarization is present. In other words, the T wave in early repolarization is usually 4 times the amplitude of the ST elevation. Another way to describe this would be that the ST elevation is less than 25% of the T wave amplitude in early repolarization.
2) The ST elevation in early repolarization resolves when the person exercises.
3) Early repolarization, unlike pericarditis, is a benign ECG finding that should not be associated with any symptoms.
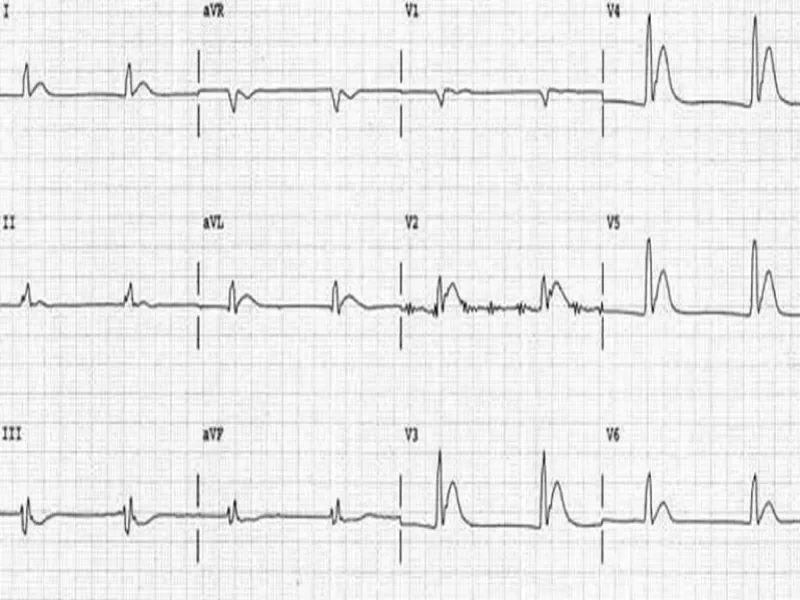
Case 19: WPWs. Right posteroseptal accessory pathway. Short PR and delta wave are evident. Q in LIII and aVF denote posteroseptal.
Case 19:
Case 20: 6 months old infant presenting with dilated cardiomyopathy. The 15 leads electrogram was obtained during the evaluation. What is your diagnosis?
Case 20:
Sinus tachycardia, rate 154/min. Cath. was done.
Anomalous left coronary artery.
Case 21: Your diagnosis please.

Case 21:
Prolonged QT, 0.50 sec. Note T wave changing morphology. Management: maximum tolerated dose of beta blockers, stop any causative drugs if any. There is also RBB.
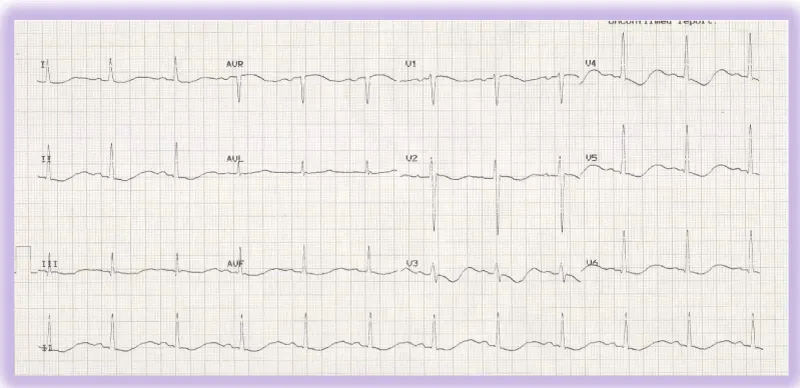
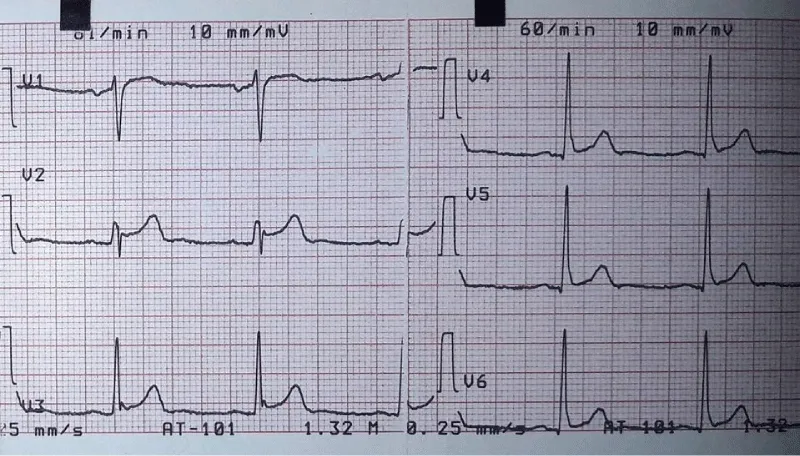
Case 22: Early repolarization syndrome: Note J point elevation in V3, 4, 5, 6. Rsr’ in V2. ST elevation with upsloping in V2, 3.
Case 22:
Early repolarization (ER), also recognized as “J-waves” or “J-point elevation”’ is an electrocardiographic abnormality consistent with elevation of the junction between the end of the QRS complex and the beginning of the ST segment in 2 contiguous leads; followed by a horizontal, downslopping or upsloping ST segment elevation or no elevation. If associated with ST elevation downslopping this is more dangerous.
| Index | |
| Case | Diagnosis |
| 1 | Atrial fibrillation; right bundle block with left axis, left anterior hemiblock |
| 2 | None sustained ventricular tachycardia |
| 3 | Wolff Parkinson White Syndrome, right posteroseptal accessory pathway |
| 4 | Ventricular tachycardia |
| 5 | AVRT, accessory pathway vs atrial flutter with 1:1 conduction |
| 6 | Supraventricular tachycardia with aberrant conduction, left anteroseptal accessory pathway. |
| Table 1 | Differentiation of wide complex tachycardia SVT with aberration vs VT |
| 7 | Supraventricular tachycardia, AVNRT |
| 8 | Supraventricular tachycardia (AVRT) with electric alternans |
| 9 | Congenital LQT Syndrome |
| 10 | Congenital LQT Syndrome |
| 11 | Acquired LQTS |
| 12 | Acquired LQTS |
| 13 | Short QT syndrome, hypercalcemia |
| 14a | Arrhythmogenic right ventricular dysplasia |
| 14b | Ventricular tachycardia in arrhythmogenic right ventricular dysplasia |
| 15 | VT in right ventricular dysplasia. |
| 16 | cardiac resynchronization pacing (biventricular pacing) |
| 17 | Pacemaker Malfunction: undersensing, |
| Table 2 | Possible Causes of undersensing |
| 18 | Acute pericarditis |
| 19 | WPWs. Right posteroseptal accessory pathway |
| 20 | Sinus tachycardia, rate 154/min in 6 months old infant. Anomalous left coronary artery. |
| 21 | Prolonged QT, 0.50 sec. |
| 22 | Early repolarization syndrome |
- Chou's Electrocardiography in Clinical Practice: Adult and Pediatric, Sixth Edition, Saunders, Philadelphia, 2008.
- Surawicz B et al. ACC/AHA recommendations for the standardization and interpretation of the electrocardiogram. Circulation. 2009; 119: e235-240.
- Zhang J, Hocini M, Strom M, Cuculich PS, Cooper DH, et al. The Electrophysiological Substrate of Early Repolarization Syndrome: Noninvasive Mapping in Patients. JACC Clin Electrophysiol. 2017 Aug; 3: 894-904. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/29130071
- Corrado D, Biffi A, Basso C, Pelliccia A, Thiene G. 12-lead ECG in the athlete: physiological versus pathological abnormalities. Br J Sports Med. 2009; 43: 669–676. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/19734501
- Basu J1, Malhotra A. Interpreting the Athlete’s ECG: Current State and Future Perspectives. Curr Treat Options Cardiovasc Med. 2018; 20: 104. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/30456469
- Zorzi A, ElMaghawry M, Corrado D. Evolving interpretation of the athlete's electrocardiogram: from European Society of Cardiology and Stanford criteria, to Seattle criteria and beyond. J Electrocardiol. 2015; 48: 283-2891. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/25724348
- Drezner JA, Sharma S, Baggish A, Papadakis M, Wilson MG, et al. International criteria for electrocardiographic interpretation in athletes: Consensus statement. Br J Sports Med. 2017; 51: 704-731. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/28258178
- Begg G, Willan K, Tyndall K, Pepper C, Tayebjee M. Electrocardiogram interpretation and arrhythmia management: a primary and secondary care survey. Br J Gen Pract. 2016; 66: e291-e296. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/27025557