
More Information
Submitted: March 16, 2023 | Approved: March 28, 2023 | Published: March 29, 2023
How to cite this article: Maturi B, Sharma A, Runkana A, Rajasekaran R, Kondapaneni V, et al. A rare case of foreign body in coronary sinus. A novel endovascular method for retrieval. J Cardiol Cardiovasc Med. 2023; 8: 039-041.
DOI: 10.29328/journal.jccm.1001151
Copyright License: © 2023 Maturi B, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Central venous catheter; Coronary sinus; Port catheter fracture; Navigational electrophysiology catheter

A rare case of foreign body in coronary sinus. A novel endovascular method for retrieval
Bhanu Maturi1* , Ashwini Sharma2, Ashok Runkana3, Rhoshini Rajasekaran1, Varshitha Kondapaneni1 and Tilachan Parajuli1
, Ashwini Sharma2, Ashok Runkana3, Rhoshini Rajasekaran1, Varshitha Kondapaneni1 and Tilachan Parajuli1
1UAB Heersink School of Medicine, Department of Internal Medicine, 2055 E south Blvd, Ste 200, Montgomery AL36116, USA
2Montgomery Cardiovascular Associates, 273 Winston M Blount loop, Montgomery, AL, 36117, USA
3Southeastern Cardiovascular Associates, 2055E South Blvd, Ste 403, Montgomery AL, 36116, USA
*Address for Correspondence: Bhanu Maturi, UAB Heersink School of Medicine, Department of Internal Medicine, 2055 E south Blvd, Ste 200, Montgomery AL36116, USA, Email: [email protected]; [email protected]
Central venous catheter fracture and migration are rare complications in patients receiving long-term infusions or chemotherapy. We present a rare case of a chest port catheter fracture that migrated into the coronary sinus. This case is likely the fourth report of a port catheter fracture with migration to the coronary sinus. Because of the difficult-to-retrieve location, multiple attempts were unsuccessful with traditional techniques using a loop snare. Finally, the fractured portion was disengaged from the coronary sinus using a navigational electrophysiology catheter guided by intracardiac echocardiography; the dislodged end was snared and eventually removed by the femoral route. This case of a chest port catheter fracture is unique because of the unusual migration to the coronary sinus and the use of a navigational electrophysiology catheter as a novel retrieval technique.
A central venous catheter is typically used to administer long-term chemotherapy or infusions. These catheters include both tunneled central venous catheters and totally implantable devices, also called ports [1]. Although a relatively safe procedure, catheterization is associated with some complications, including extravasation, rupture, thrombosis, and infection. A rupture with subsequent migration is rare, occurring in 0.5% – 3.0% of cases [2]. Rupture can occur spontaneously or during catheter removal [3]. Common sites of migration include the superior vena cava, inferior vena cava, right heart, right ventricle, and pulmonary arteries, whereas migration to the coronary sinus is very rare [4,5]. To date, only three cases of migration to this site have been reported. Management consists of percutaneous retrieval in most cases; open thoracotomy or long-term warfarin treatment is rarely required. Among these cases, percutaneous transcatheter removal has become the standard of care.
A 24-year-old woman with immune thrombocytopenia managed with intravenous immunoglobulin infusions through a chest port catheter was admitted to our emergency room after experiencing chest discomfort with sudden onset while receiving the infusion. She did not appear to be in any acute distress and her vital signs were stable. Electrocardiography was unremarkable. Laboratory tests showed troponin values within the normal range. Further workup with chest radiography revealed that the chest port catheter was fractured and had migrated to the right atrium (Figure 1).
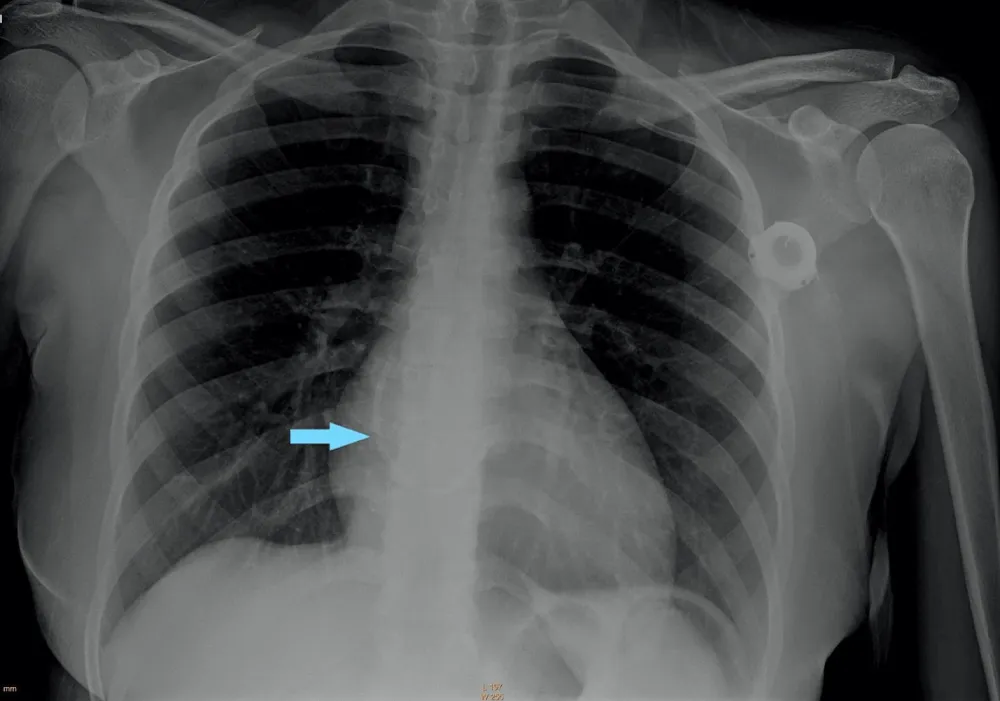
Figure 1: Chest radiography shows a fractured chest port catheter in the right atrium (blue arrow).
The patient underwent chest computed tomography, which showed that the fractured port migrated to the coronary sinus area of the right atrium (Figure 2).
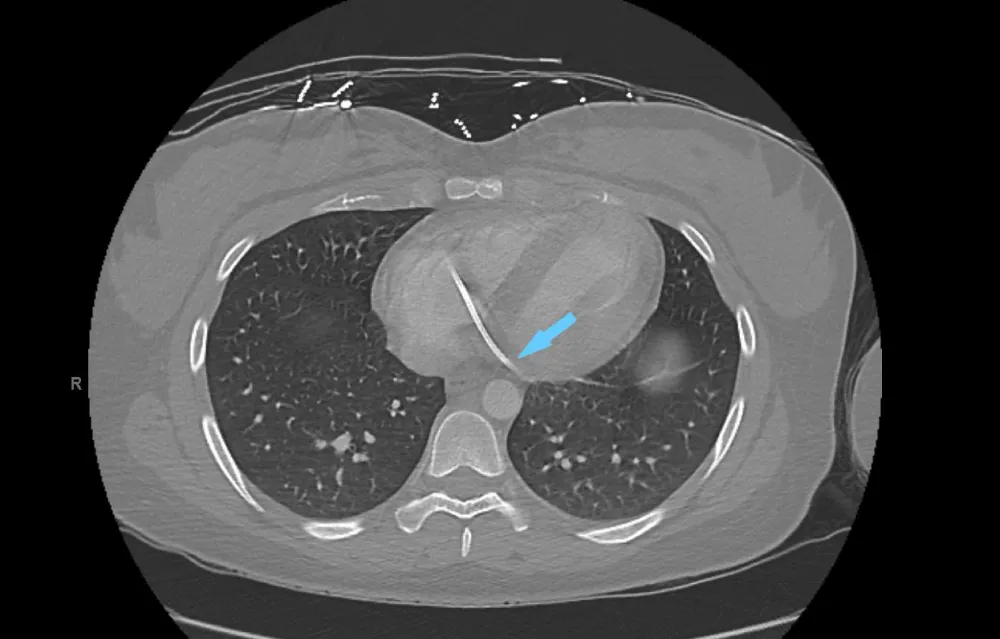
Figure 2: Computed tomography of the chest shows a fractured port in the coronary sinus of the right atrium (blue arrow).
Electrophysiologist and Interventional Cardiology were consulted, and in a coordinated approach, the patient underwent right heart catheterization using an ultrasound-guided right femoral venous access. Multiple retrieval attempts were made using an endovascular loop snare and various catheters, without success in reaching the proximal end of the port. Subsequently, an intracardiac echocardiography catheter was advanced and confirmed that one end of the port was lodged deep in the coronary sinus and the other end had traversed the tricuspid valve and was lodged into the posterior wall of the right atrium.
Therefore, further retrieval attempts using multiple catheters to hook the port over the tricuspid valve were unsuccessful. Finally, a navigational electrophysiology steerable catheter was used to hook the port over the tricuspid valve (Figure 3 and Video 1 Click here.
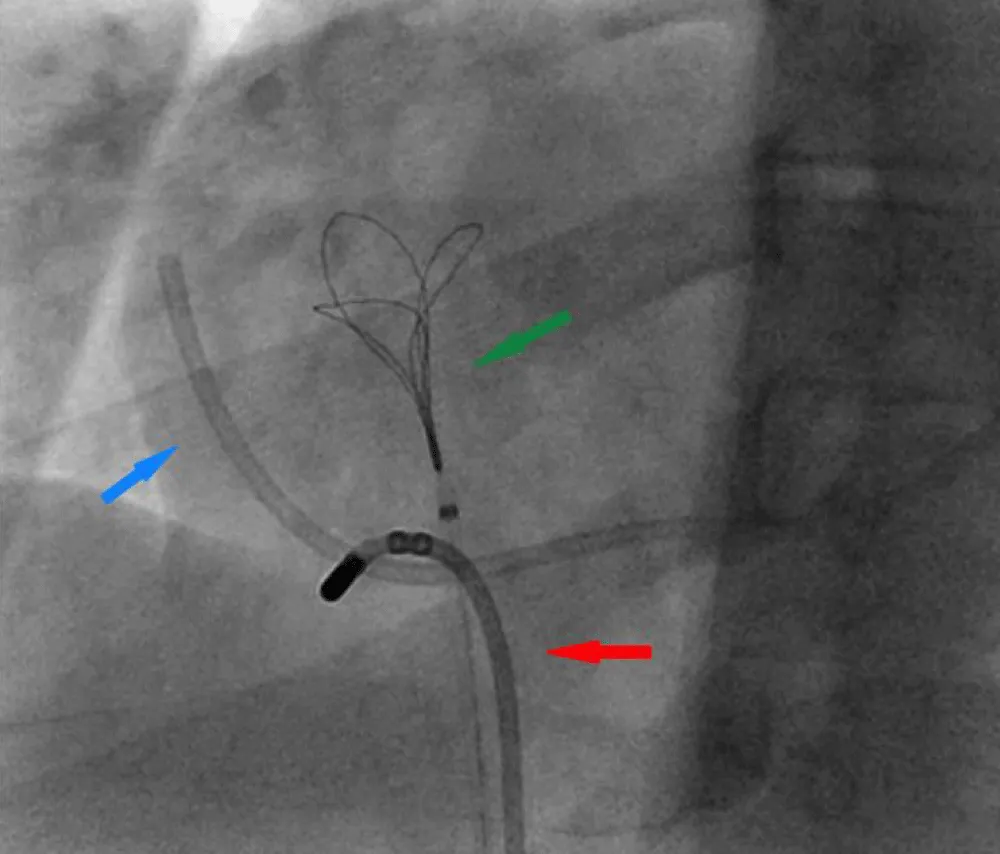
Figure 3: Right Heart catheterization shows a Navigational steerable catheter hooking the port and disengaging it from the coronary sinus. Fractured Port (blue arrow), Navigational steerable catheter (red arrow), Snare (green arrow).
This maneuver freed the right atrial end of the port, for which the endovascular snare was then used with success. The fractured port was finally retrieved as one unit (Figure 4 and Video 2 Click here.
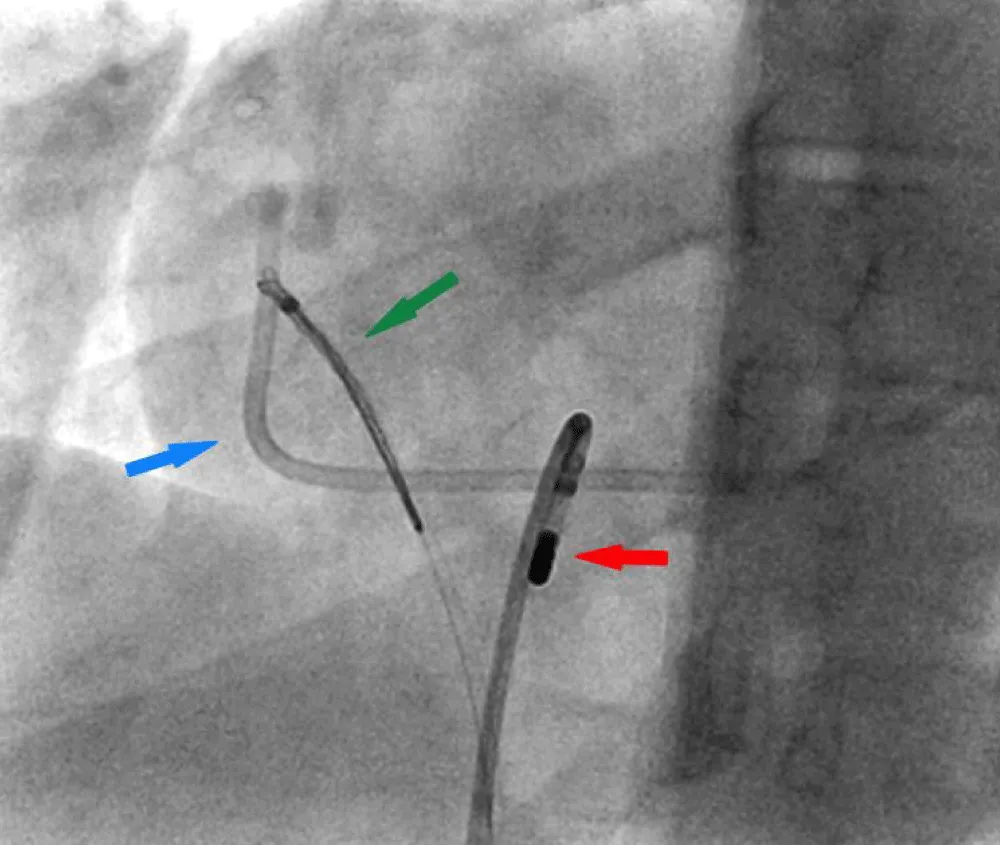
Figure 4: Right Heart catheterization showing Endovascular snare retrieving the freed end of the port. Fractured Port (blue arrow), Navigational steerable catheter (red arrow), Snare (green arrow).
The patient had an uneventful perioperative period and later underwent complete extraction of the port remnants.
Central venous catheters are widely used for patient resuscitation and for the administration of medications, chemotherapy, and parenteral nutrition. Despite care during insertion and maintenance periods, complications associated with venous port devices are inevitable. Immediate complications include pneumothorax, hemorrhage, arterial puncture, air embolism, and arrhythmias. Late complications include thrombosis, infection, catheter fracture, and migration. Cardiac migration is rare and occurs in only 0.1% – 1% of cases [6]. This type of migration is associated with severe and sometimes fatal complications, such as arrhythmias, rupture, and valve closure. Most often the fragments lodge into the right heart chambers or pulmonary arteries. The migration of the fractured port into the coronary sinus is highly uncommon because of the anatomic location of the ostium and the Thebesian valve guarding it. To date, only three cases have been reported [7-9]. Foreign bodies in the Coronary sinus can be asymptomatic but, in some cases lead to precordialgia, pericardial effusion, ST elevation, and thrombus with associated embolization.
The “pinch-off sign” in catheterization has been described as a leading cause of port fracture in some cases. When the catheter is placed using a puncture medial to the midclavicular line, the catheter travels through the costoclavicular space adjacent to the subclavian vein rather than into the subclavian vein itself, making the catheter more susceptible to compression during shoulder movement [10]. It is recommended to insert the catheter lateral to the midclavicular line. All port fractures must be removed as soon as possible. The percutaneous approach is preferred because it is simple and less invasive. The pathophysiology associated with coronary sinus thrombus is related to endothelial injury caused during migration. In some cases, even the retrieval process is associated with endothelial injury and thrombus which should be considered cautiously during retrieval. An extensive literature search showed that the use of loop snares has been successful for the retrieval of port fractures in most cases. In rare instances, baskets, forceps, and a pigtail catheter were required [4,5]. The need for surgical removal or long-term warfarin treatment is also rare.
The present case presents a difficult setting in which one end of the catheter is deep in the coronary sinus and the other end is in the traverses of the tricuspid valve. This novel retrieval technique used in this case is of great interest. Guidance by intracardiac echocardiography and the use of a navigational electrophysiology catheter to dislodge the tip from the coronary sinus provides a unique way to precisely navigate to a difficult-to-reach foreign body in the coronary sinus.
Challenges occur during the extraction of port fractures from difficult-to-reach areas such as the coronary sinus. Our groundbreaking method of using a navigational electrophysiology catheter to dislodge the port fracture from the coronary sinus paves the way for its potential use in difficult cases in the future.
Ethics statement
The authors declare that the work described has been carried out in accordance with The Code of Ethics of the World Medical Association (Declaration of Helsinki) for experiments involving humans.
Consent statement
Complete written informed consent was obtained from the patient (or appropriate parent, guardian, or power of attorney) for the publication of this study and accompanying images.
- Gazzanelli S, Miccini M, Sapienza P, Cavallaro G, Biacchi D, Crocetti D, Fiori E, Sammartino P, Guerra C, Ranieri MV. Fracture and migration in right atrium of a permanent venous central access system in a elderly patient: case report and literature review. Clin Ter. 2022 May 25;173(3):207-213. doi: 10.7417/CT.2022.2419. PMID: 35612331.
- Kock HJ, Pietsch M, Krause U, Wilke H, Eigler FW. Implantable vascular access systems: experience in 1500 patients with totally implanted central venous port systems. World J Surg. 1998 Jan;22(1):12-6. doi: 10.1007/s002689900342. PMID: 9465755.
- Hamilton HC, Foxcroft DR. Central venous access sites for the prevention of venous thrombosis, stenosis and infection in patients requiring long-term intravenous therapy. Cochrane Database Syst Rev. 2007 Jul 18;(3):CD004084. doi: 10.1002/14651858.CD004084.pub2. Update in: Cochrane Database Syst Rev. 2012;3:CD004084. PMID: 17636746.
- Cheng CC, Tsai TN, Yang CC, Han CL. Percutaneous retrieval of dislodged totally implantable central venous access system in 92 cases: experience in a single hospital. Eur J Radiol. 2009 Feb;69(2):346-50. doi: 10.1016/j.ejrad.2007.09.034. Epub 2007 Oct 31. PMID: 17976941.
- Bessoud B, de Baere T, Kuoch V, Desruennes E, Cosset MF, Lassau N, Roche A. Experience at a single institution with endovascular treatment of mechanical complications caused by implanted central venous access devices in pediatric and adult patients. AJR Am J Roentgenol. 2003 Feb;180(2):527-32. doi: 10.2214/ajr.180.2.1800527. PMID: 12540466.
- Andris DA, Krzywda EA, Schulte W, Ausman R, Quebbeman EJ. Pinch-off syndrome: a rare etiology for central venous catheter occlusion. JPEN J Parenter Enteral Nutr. 1994 Nov-Dec;18(6):531-3. doi: 10.1177/0148607194018006531. PMID: 7602729.
- Karam AR, Hourani MH, Al-Kutoubi AO. Catheter fracture and migration into the coronary sinus--an unusual migration site: case report and review. Clin Imaging. 2009 Mar-Apr;33(2):140-3. doi: 10.1016/j.clinimag.2008.10.001. PMID: 19237059.
- Arnould MA, Blanchard D. Catheter migration after fracture is not always in right cavities. Cardiovasc Interv Ther. 2013 Jan;28(1):119-22. doi: 10.1007/s12928-012-0127-y. Epub 2012 Oct 13. PMID: 23065411.
- Pignataro BS, Nishinari K, Wolosker N, Bomfim GA. Fracture and migration into the coronary sinus of a totally implantable catheter introduced via the right internal jugular vein. BMJ Case Rep. 2014 Dec 1;2014:bcr2014207276. doi: 10.1136/bcr-2014-207276. PMID: 25452299; PMCID: PMC4256600.
- Aitken DR, Minton JP. The "pinch-off sign": a warning of impending problems with permanent subclavian catheters. Am J Surg. 1984 Nov;148(5):633-6. doi: 10.1016/0002-9610(84)90340-4. PMID: 6496853.