More Info
Author's satisfaction with
- Friendly and hassle-free publication process
- Less production time of articles
- Constructive peer-review
- Enhancing journal reputation
- Regular feedback system
- Quick response to authors' queries
Recently Viewed
Most Viewed
Clinical Images
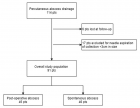
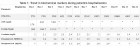


Table of Contents

Conservative treatment versus invasive approach in elderly patients with myocardial infarction without ST-segment elevation
Published on: 30th April, 2020
OCLC Number/Unique Identifier: 8588723372
Myocardial infarction without ST segment elevation is one of the most common causes of hospitalization of the elderly patient [1]. Coronarography followed by revascularization, is performed in the vast majority of cases of myocardial infarction without ST segment elevation, in the regions with a well-developed health system. The decision to perform the procedure, the type of approach (early/late) and the selection of the type of myocardial revascularization depend on numerous factors such as: associated comorbidities, clinical presentation, the risk group in which the patient is framed, fragility, cognitive status, life expectancy etc. [2,3]. Older patients often present with various comorbidities, having a higher risk of complications and an unfavorable evolution. Thus, it was observed that invasively treatment is less commonly used in elderly patients with comorbidities, even if, the current guideline recommends that the invasive strategy should be considered in all patients with NSTEMI, regardless of age. At the same time, this subgroup of patients is not so well represented in the studies performed so far, the type of treatment chosen, being most often at the discretion of the attending physician [1,2].
Objective The present study aims to analyze the evolution of a subgroup of patients ≥ 70 years of age, with different comorbidities, with the diagnosis of myocardial infarction without ST segment elevation, according to the type of treatment applied: conservative versus invasive strategy (diagnostic coronarography ± revascularization, if appropriate).
Effects of highest dose of sacubitril/valsartan association compared to lower doses on mortality and ventricular arrhythmias
Published on: 24th April, 2020
OCLC Number/Unique Identifier: 8588720714
Background: Sudden cardiac death is a major healthcare issue in reduced ejection fraction heart failure (HFrEF) patients. Recently, the new association of sacubitril/valsartan showed a reduction of both ventricular arrhythmias (VA) and mortality even at low dose compared to enalapril in HF patients. The purpose of our study was to assess whether the highest dose of sacubitril/valsartan compared to lower doses may improve the rate of death and VA in a population of patients with HFrEF and with an implantable cardiac defibrillator (ICD).
Methods: 104 HF patients with reduced EF under sacubitril/valsartan with an ICD were divided in 2 groups: the first one with the lower doses of sacubitril/valsartan (24/26 mg or 49 mg/51 mg twice daily) and the second with the maximal dose (97mg/103mg twice daily). The primary outcome was a composite of death or appropriate ICD therapy for VA.
Results: After a median follow-up of 14 months, 39 patients were treated with lower doses and 65 patients with the highest dose. Patients from the lower doses group were older (70 [60-80] vs. 66 [60-70]; p = 0,03), more symptomatic at initiation (NYHA 3: 44% vs. 19%; p < 0,01) and more often in atrial fibrillation (31% vs. 12%; p = 0,04). The primary composite endpoint occurred in 14 patients (36%) in the low doses group versus 7 patients (11%) in high dose group (p < 0,01). This difference was particularly observed in the subgroup of patients with ischemic cardiomyopathy. In a multivariable analysis, the higher dose was independently associated with the primary outcome with an HR = 2,934 [IC 95% 1,147 – 7,504]; p = 0,03. Kaplan-Meier curve showed an early effect of the highest dose of sacubitril/valsartan association.
Conclusion: Patients with HFrEF under the highest dose of sacubitril/valsartan showed better clinical outcomes with a decrease of both mortality or appropriated ICD therapies related to ventricular arrhythmias.
Glycosaminoglycans as Novel Targets for in vivo Contrast-Enhanced Magnetic Resonance Imaging of Atherosclerosis
Published on: 20th April, 2020
OCLC Number/Unique Identifier: 8588716816
Atherosclerosis is an important promoter of cardiovascular disease potentiating myocardial infarction or stroke. Current demand in biomedical imaging necessitates noninvasive characterization of arterial changes responsible for transition of stable plaque into rupture-prone vulnerable plaque. in vivo contrast enhanced magnetic resonance (MR) imaging (MRI) allows quantitative and functional monitoring of pathomorphological changes through signal differences induced by the contrast agent uptake in the diseased vessel wall, therefore it is the ideal modality toward this goal. However, studies have so far focused on the cellular targets of persisting inflammation, leaving extracellular matrix (ECM) far behind. In this review, we portray ECM remodeling during atherosclerotic plaque progression by summarizing the state of the-art in MRI and current imaging targets. Finally, we aim to discuss glycosaminoglycans (GAGs) and their functional interactions, which might offer potential toward development of novel imaging probes for in vivo contrast-enhanced MRI of atherosclerosis.
Recurrence of atrial fibrillation after pulmonary vein isolation, should we change the energy and technique?
Published on: 3rd April, 2020
OCLC Number/Unique Identifier: 8576354289
Background: Pulmonary vein isolation (PVI) is the accepted standard nowadays for atrial fibrillation (AF) ablation. The most widespread ablation techniques are cryoballoon (CB) and point-by-point radiofrequency (RF) ablation. Comparative studies between both techniques have shown their equivalence for the first ablation procedure, but no trial has explored the potential incremental benefit of crossing over the ablation technique after AF recurrence.
Objective: To explore the potential incremental benefit of a crossover ablation strategy for AF recurrences, comparatively with repeating the same ablation energy used for the first procedure.
Methods: Retrospective analysis of patients undergoing a second AF ablation procedure after documented AF recurrence. Patients were excluded if all 4 PV were isolated at the beginning of the second procedure or extra-PVI ablation was used for the second procedure. Crossover group (n = 16) included patients in which two different techniques were used for the first and second procedure (CB-RF or RF-CB). Control group (n = 23) for those with same ablation procedure (RF-RF of CB-CB). Acute procedure end-point was PVI of all four pulmonary veins. Patients were followed-up at 3, 6, and 12 months with an electrocardiogram and a 24 h-holter. Arrhythmia-free survival at 1 year after the second ablation procedure was studied, comparing efficiency and safety of the two approaches (crossover vs. same energy). Success was defined as freedom from AF or atrial tachycardia lasting > 30 s off antiarrhythmic drugs (AADs)
Results: A cohort of 39 paroxysmal and persistent AF patients was analyzed. PVI after the second procedure was 100% in all patients in both groups. There were no baseline relevant differences between the two groups. No deaths or hospitalizations occurred during follow up (data censored at 24h moths). At 1 year, arrhythmia free-survival was significantly higher in the crossover group compared to control group [93,3% vs. 47,8%; HR 0.19 (0.06-0.66);p = 0,009].
Conclusion: Crossing the ablation technique (point-by-point radiofrequency or cryoballoon PVI) after AF recurrence significantly improved arrhythmia free-survival at one year, despite no difference in acute success (PVI isolation). Randomized controlled trials with a higher amount of patients are needed to confirm the results and widespread this approach.
Primary prevention of SCD with ICD in the elderly
Published on: 30th March, 2020
OCLC Number/Unique Identifier: 8576353351
Implantable cardioverter defibrillators (ICDs) are electronic devices that can prevent sudden cardiac death (SCD) caused by arrhythmic events in patients.
The latest ESC/EAS and ACC/AHA Guidelines deem the placement of an ICDs appropriate in patients with heart failure class NYHA II and III in the presence of an ejection fraction less than or equal to 35% [1,2]. ICDs are usually not indicated in either class I or IV patients. The Guidelines recommendations for primary prevention of SCD with ICD implantation do not take into account the age of the patients but only their life expectancy which must be at least 1 year.
Our patients usually are over eighty years old with heart failure and severely reduced ejection fraction. We must consequently decide if it is right to implant these patients with an ICD. Is the use of ICD in the patients over 80, in particular over 90 years old, really make sense becomes particularly important considering demographic changes that await us in the coming decades.
Dapt Review
Published on: 25th March, 2020
OCLC Number/Unique Identifier: 8576364795
Dual antiplatelet therapy (DAPT) combining aspirin and a P2Y12 receptor inhibitor has been consistently shown to reduce recurrent major adverse cardiovascular events (MACE) in patients with acute coronary syndrome (ACS) or undergoing percutaneous coronary intervention (PCI) for stable coronary artery disease (CAD) compared with aspirin monotherapy but at the expense of an increased risk of significant bleeding. Among patients with stable CAD undergoing PCI with drug-eluting stents (DES), shorter duration of DAPT (3–6 months) were shown non-inferior to 12 or 24 months duration concerning MACE but reduced the rates of major bleeding? Contrariwise, prolonged DAPT durations (18–48 months) reduced the incidence of myocardial infarction and stent thrombosis, but at the cost of an increased risk of majör bleeding and all-cause mortality. Until more evidence becomes available, the choice of optimal DAPT regimen and duration for patients with CAD requires a tailored approach based on the patient clinical presentation, baseline risk profile and management strategy. Patients with acute coronary syndromes (ACS) and a history of atrial fibrillation (AF) have indications for both dual antiplatelet therapy (DAPT) and oral anticoagulation (OAC). Triple therapy (TT), the combination of DAPT and OAC, is recommended in guidelines. This article provides a contemporary state-of-the-art review of the current evidence on DAPT for secondary prevention of patients with CAD and its future perspectives.
A study on pacemaker pocket infection
Published on: 25th March, 2020
OCLC Number/Unique Identifier: 8576354340
Objective: Cardiac implantable electronic device (CIED) infections now constitute ∼ 10% of all endocarditis cases. The incidence of CIED infection is usually < 2%. Our objective was to study pacemaker pocket infection rate and different risk factors in our institution.
Methods: This observational study was conducted over a period of five years from January 2011 to December 2016 and it included 1096 patients. Common risk factors like patients with diabetes, repeat procedure, chronic renal failure, chronic obstructive airway disease, immunosuppressive agents were studied in our patients.
Results: Our study consisted of 1096 patients. Pacemaker pocket infection occurred in sixteen patients (1.5%). Chronic renal failure patients were one hundred thirty in our study (11.86%). There were three hundred fifty six diabetic patients (32.48%). Repeat procedure was done in ninety five patients (8.6%).
Results: Our study consisted of 1096 patients. Pacemaker pocket infection occurred in sixteen patients (1.5%). Chronic renal failure patients were one hundred thirty in our study (11.86%). There were three hundred fifty six diabetic patients (32.48%). Repeat procedure was done in ninety five patients (8.6%)
Eighty six patients were suffering from chronic obstructive airway (7.8%). Patients on immunosuppressive therapy were fourteen in our study (1.2%).
Conclusion: Pacemaker pocket infections is a dreaded complication after pacemaker implantation. During implantation, there is a risk of device contamination with the patient’s own skin flora and it can be prevented by ideal surgical asepsis technique, pre and perioperative use of antibiotics.
Clinical relevance linked to echocardiography diagnosis in Bland, White and Garland syndrome
Published on: 6th March, 2020
OCLC Number/Unique Identifier: 8560715071
Introduction: Bland, White and Garland syndrome is a coronary anomaly with high mortality without treatment. Its clinical presentation is varied which makes epidemiological documentation difficult. Echocardiography is a useful non-invasive tool for diagnosis.
Objective: To determine the echocardiographic variables that lead to the diagnosis of Bland, White and Garland syndrome and their clinical relevance.
Material: Observational, prospective and cross-sectional study in 31 patients of the “William Soler” Pediatric Cardiocenter, from 2005 to 2018. To check the association of echocardiographic variables with the diagnosis of Bland, White and Garland syndrome, an effectiveness study was carried out that included the analysis of the incidence of echocardiographic variables that lead to the diagnosis of this entity. The clinical relevance was estimated according to the minimum importance limit. The statistical validation of the research results adopted a significance level of less than 5% (p < 0.05).
Results: The variables that facilitate the echocardiographic diagnosis of Bland, White and Garland syndrome were the echocardiographic visualization of the anomalous connection and the reversed flow in the anomalous left coronary artery. These echocardiographic measures have clinical relevance according to the quantification of risk estimators (incidence) the echocardiographic visualization of the anomalous connection, RR 39.00 and the reversed flow in the anomalous coronary artery, RR 26.31. LIM´s calculation value amounted to 6.31 and coincided with the risk estimators (incidence).
Conclusion: The echocardiographic visualization of the anomalous origin of the left coronary artery from the pulmonary arterial trunk and the detection of the local intracoronary reversed flow instituted as factors to be considered for the effective diagnosis of the disease. The documentation of the diagnostic aspects of the syndrome through echocardiography contains high statistical value and clinical relevance.
Pathological left ventricular hypertrophy and outflow tract obstruction in an infant of a diabetic mother: A case report
Published on: 3rd March, 2020
OCLC Number/Unique Identifier: 8560717043
Background: Infants of diabetic mothers (IDMs) are at increased risk of developing congenital anomalies including cardiac defects. Pathological left ventricular hypertrophy, asymmetrical septal hypertrophy and outflow tract obstruction is a rare but known cardiac comorbidity in infants of diabetic mothers. The severity of this condition in IDMs can vary from an incidental finding on echocardiography to an infant with severe symptoms of congestive heart failure and specific management of the condition varies.
Aim: The aim of this article is to report this clinical entity in a Nigerian infant born to a mother with poor glycaemic control in pregnancy and highlight management.
Case report: We report a term neonate who was diagnosed as a case of pathological left ventricular hypertrophy, asymmetrical septal hypertrophy and outflow tract obstruction delivered to a mother with gestational diabetics with poor glycaemic control in pregnancy. Child was treated successfully with β-adrenergic blocker and showed resolution of hypertrophy in follow-up echocardiography.
Conclusion: Infants of diabetic mothers are very high risk infants. Pathological left ventricular hypertrophy in IDM have good prognosis. Early recognition and prompt intervention is advocated.
His bundle pacing in heart failure: A review of current literature
Published on: 3rd March, 2020
OCLC Number/Unique Identifier: 8560715663
Biventricular (BiV) pacing revolutionized the heart failure management in patients with sinus rhythm and left bundle branch block; however, left ventricular-lead placement is not always technically possible. Also, BiV pacing does not fully normalize ventricular activation and, therefore, the ventricular resynchronization is imperfect. On the other hand, right ventricular pacing for bradycardia may cause or worsen heart failure in some patients by causing dyssynchronous ventricular activation. His bundle pacing comes as an alternative to current approaches as it activates the ventricles via the native His-Purkinje system, resulting in true physiological pacing, and, therefore, is a promising site for pacing in bradycardia and traditional CRT indications in cases where it can overcome left bundle branch block. Furthermore, it has the potential to open up new indications for pacing therapy in heart failure, such as targeting patients with PR prolongation, but a narrow QRS duration. In this article we explore the history, clinical evidence, proposed mechanisms, procedural characteristics, and the role in current therapy of His bundle pacing in the prevention and treatment of heart failure.
ECG interpretation and commentary
Published on: 18th February, 2020
OCLC Number/Unique Identifier: 8550965055
This is demonstration of selected ECGs for learning or for exams; guided by lessons from great teachers as Prof. Hein Wellens MD. Here we provide advanced examples with comment and analysis.
Localization of the occluded vessel in acute myocardial infarction
Published on: 18th February, 2020
OCLC Number/Unique Identifier: 8550958571
This is a review of features in ECG to diagnose the culprit artery responsible for the infarction. Localization of the occluded vessel in acute myocardial infarction is important for many reasons: to know which artery is to dilate and stent; to assess the severity of the lesion; to compare with the echocardiographic area with hypokinesia or akinesia and to differentiate the recent from the old occluded vessel. The ST-segment changes in 12-lead ECG form the basis of diagnosis, management, and prognosis.
Angiotensin II type 1 receptor and the activation of Myosin Light-Chain Kinase and Protein Kinase C-βII: Mini Review
Published on: 17th February, 2020
OCLC Number/Unique Identifier: 8534733539
The involvement of the angiotensin II type 1 receptor in the Frank-Starling Law of the Heart, where the various activations are very limited, allows simple analysis of the kinase systems involved and thence extrapolation of the mechanism to that of angiotensin control of activation of cardiac and skeletal muscle contraction. The involvement of phosphorylation of the myosin light chain in the control of contraction is accepted but not fully understood. The involvement of troponin-I phosphorylation is also indicated but of unknown mechanism. There is no known signal for activation of myosin light chain kinase or Protein Kinase C-βII other than Ca2+/calmodulin but the former is constitutively active and thus has to be under control of a regulated inhibitor, the latter kinase may also be the same. Ca2+/calmodulin is not activated in Frank-Starling, i.e. there are no diastolic or systolic [Ca2+] changes. I suggest here that the regulated inhibition is by myosin light chain phosphatase and/or β-arrestin. Angiotensin activation, not involving G proteins. is by translocation of the β-arrestin from the sarcoplasm to the plasma membrane thus reducing its kinase inhibition action in the sarcoplasm. This reduced inhibition has been wrongly attributed to a mythical downstream agonist property of β-arrestin.
Gender-specific associations of anthropometric measures of adiposity with blood pressure and hypertension in young Chinese Medical College Students
Published on: 31st January, 2020
OCLC Number/Unique Identifier: 8535882054
Purpose: There are uncertainties about whether general or central obesity is the more important determinant for blood pressure and hypertension in young Chinese. We aim to investigate the association between adiposity measures and blood pressure and hypertension in young medical students.
Methods: A total of 380 medical students were recruited from the 2012 batch in the Clinical College of Dali University. Anthropometric measures and office blood pressure were measured. Blood pressure status was defined by Chinese hypertension guidelines and ACC/AHA 2017 hypertension guidelines, respectively. We examined the associations of adiposity measures (body weight, body mass index [BMI], waist circumference, hip circumference, waist-to-hip ratio [WHR], waist-to-height ratio [WHtR], ponderal index [PI], body adiposity index (BAI) and conicity index [CI]) with blood pressure and hypertension by sex.
Results: In 380 subjects (women 66.6%, mean age 21.5 years), the prevalence of obesity (BMI ≥ 28 kg/m2) was 2.1%, and the prevalence of hypertension was 2.6% (≥ 140/90 mmHg) and 24.5% (≥ 130/80 mmHg), respectively. In correlation analyses and multivariable-adjusted linear regression analyses, most adiposity measures of central obesity were significantly associated with blood pressure in men, while in women, either adiposity measures of central or general obesity were associated with blood pressure. The predictive power of adiposity measures for hypertension was generally low in men. However, adiposity measures of either general obesity or central obesity were predictive for hypertension defined by Chinese hypertension guidelines in women.
Conclusion: There are gender-specific associations of central and general obesity with blood pressure and hypertension in young Chinese medical students.
Occluded superior vena cava and failed epicardial pacing: An unorthodox solution
Published on: 13th January, 2020
OCLC Number/Unique Identifier: 8514668207
Permanent pacemaker implantation is conventionally done via upper limb veins. But in 1% - 6% cases, usual sub clavicular approach is either not possible or contraindicated due to complete occlusion of superior vena cava (SVC) or bilateral subclavian vein and/or bilateral implant site infection or thin skin [1]. Alternative approaches are warranted, including leadless pacemaker or complex lead extraction techniques, before considering surgical epicardial lead placement as a last resort because it has own hazards. We report a patient with complete heart block, total SVC obstruction, and a previously implanted malfunctioning epicardial lead presenting with pacemaker end of life. In view of exhaustion of the surgical option and in a resource constrained situation for lead extraction or leadless pacemaker, transiliac endocardial pacemaker implantation was done and a repeat surgery was averted.
Learning objective: Complete venous occlusion is not very often encountered after pacemaker/ICD implantation. Apart from the risk of general anesthesia and invasive surgery, epicardial leads increase battery drain, and have a shorter operating life compared to an endocardial lead. The sparingly utilized iliac venous approach for permanent pacemaker implantation is a valuable, safe and minimally invasive alternative, when the conventional percutaneous access is unavailable, and surgery is undesirable or not possible.
Coronary-intercostal steal syndrome, a rare connection between the left circumflex coronary artery and intercostal arteries: A case report
Published on: 13th January, 2020
OCLC Number/Unique Identifier: 8514666304
A 60-year-old female patient presented with typical anginal pain on exertion and relieved by rest for about one month. Percutaneous coronary angiography was done and showed an abnormal left circumflex coronary artery connecting to intercostal artery. Embolization of that abnormal connection was done successfully and the patient discharged from hospital after 24 hours. This case shows a new form of coronary steal syndrome. This cause could be missed if not put under the differential diagnosis of typical anginal pain with normal coronary arteries.
Effect of hemodialysis session on acute changes in inflammatory and cardiovascular risk biomarkers
Published on: 9th January, 2020
OCLC Number/Unique Identifier: 9269418657
Background: Inflammation is associated with enhanced cardiovascular risk profile and increased cardiovascular mortality in end-stage kidney disease patients undergoing hemodialysis. Mechanisms of activated acute phase reaction in patients on chronic hemodialysis remain to be identified. As successful treatment of the inflammatory condition in these patients may improve long-term survival, we studied potential changes in different inflammatory biomarkers of cardiovascular risk in end-stage kidney disease patients after a mid-week hemodialysis session.
Methods: Inflammatory biomarkers of cardiovascular risk (cystatin-C, homocysteine, C-reactive protein, procalcitonin, pentraxin-3, serum amyloid-A) and atherogenic plasma lipoproteins (Lipoprotein(a), cholesterol low and high density lipoproteins) were studied in 21 end-stage kidney disease patients previously and after a mid-week hemodialysis session.
Results: We found a significant reduction in serum levels of low molecular weight molecules: cystatin-C (5.56 to 1.85 mg/L, 66.73%, p < 0.001), homocysteine (22.85 to 13.25 µmol/L, 42.01%, p < 0.001) and procalcitonin (0.788 to 0.457 ng/mL, 42.01%, p < 0.001). Large molecules as C-reactive protein (9.70 to 9.90 mg/L, 2.06%, p = 0.022) and pentraxin-3 (1.67 to 4.28 ng/mL, 156%, p < 0.001) increased, but serum amyloid-A decreased (15.90 to 12.70 mg/L, 20.13%, p < 0.05). There was no change in Lipoprotein (a) levels.
Conclusion: Pentraxin-3 was a more specific inflammatory vascular marker than C-reactive protein, and the best inflammatory marker associated with hemodialysis. Homocysteine, procalcitonin and the other small proteins could be released and removed during hemodialysis session. Further studies are needed to understand the behavior and significance of these markers after successive hemodialysis.
A proposed mechanism to explain increases in intracranial pressure: The concept of cerebral artery wedge pressure
Published on: 8th January, 2020
OCLC Number/Unique Identifier: 8514665738
We hypothesize that, with elevated cerebral spinal fluid (CSF) pressure, cerebral micro-vascular obstruction and congestion may occur despite (subdural) large-vein pressures being normal. Smaller veins emptying into these larger, dura-enveloped veins are not immune to the compressive effects of elevated CSF pressure and a “Starling Resistor” mechanism might explain why elevated CSF pressures collapse these smaller veins. This small cerebral venous starling resistor compression mechanism may be the final common pathway for many patients suffering from increased CSF pressures and might also be an important contributor to impaired focal venous drainage presenting as a headache with normal venous sinus pressures.
Contact
Select by Volume & Issue
Most Viewed Keywords
- Feature selection
- Agranulocytosis
- Morbidly adherent placenta
- Rehabilitation program
- Child neglect
- Erectile dysfunction
- First depressive episode
- Hydroxychloroquine
- Hyperleukocytosis
- Complementary feeding
- School
- COVID-19
- Cancer
- Undernourished
- Alpha particles
- Methodological approaches
- HFpEF
- OD Tacrolimus
- Pain management
- Elbow hemiarthroplasty
University/Institution
Select and search by University/Institution.
Articles by Country
Select and search by country to get related articles.













Testmonials

I would like to thank JPRA for taking this decision. I understand the effort it represents for you. I'm truly happy to have the paper published in JPRA. And I'll certainly consider JPRA for my next publications as I was satisfied of the service provided, the efficiency and promptness of the interactions we had.
Emmanuel BUSATO
Publishing with the International Journal of Clinical and Experimental Ophthalmology was a rewarding experience as review process was thorough and brisk. Their visibility online is second to none as their published articles appear in all search engines. I will encourage researchers to publish with them.
Elizabeth Awoyesuku
“The choice to submit the forensic case study to the Journal of Addiction Therapy and Research was dictated by the match between the content and the potential readership. The publication process proved to be expedient and we were provided with constructive feedback from reviewers. The final article layout is attractive and conforms to standards. All-in-all, it has been a rewarding process.”
Elisabeth H Wiig
Archives of Vascular Medicine is one of the top class journal for vascular medicine with highly interesting topics. You did a professional and great Job!
Elias Noory
Thank you very much. I think the review process and all of what concerns the administration of the publication concerning our paper has been excellent. The nice and quick answers have been very good I think.
Doris Nilsson
Journal of Pulmonary and Respiratory Research is good journal for respiratory research purposes. It takes 2-3 weeks maximum for review of the manuscript to get published and any corrections to be made in the manuscript. It needs good articles and studies to get publish in the respiratory medicine. I am really glad that this journal editors helped me to get my case report published.
Divya Khanduja
Thanks you and your colleague for the great help for our publication. You always provide prompt responses and high quality of service. I am so happy to have you working with me. Thanks again!
Diana (Ding) Dai
Service and process were excellent as was the “look” of the article when published.
Deane Waldman
Great, thank you! It was very efficient working w/ your group. Very thorough reviews (i.e., plagiarism, peer, etc.). Would certainly recommend that future authors consider working w/ your group.
David W Brett
Your services are very good
Chukwuka Ireju Onyinye
I very much appreciate the humanitarian services provided in my stead by this journal/publisher. It exhibits total absence of editorial impertinence. As an Author, I have been guided to have a fruitful experience. The editorial care is highly commendable.
Chrysanthus Chukwuma
"An amazing experience with the Journal of Advanced Pediatrics and Child Health. Very fast blind review with pertinent corrections and suggestions. I highly recommand both the journal and the editor."
Chaimae Khairoun
The submission is very easy and the time from submission to response from the reviewers is short. Correspondence with the journal is nice and rapid.
Catrin Henriksson
The Clinical Journal of Obstetrics and Gynecology is an open access journal focused on scientific knowledge publication with emphasis laid on the fields of Gynecology and Obstetrics. Their services toward us have been encouraging through their kindness and respect. Great consideration has been given to us as young budding researchers and we are very grateful for this.
Carole Assontsa
During the process your positive communication, prompt feedback and professional approach is very highly appreciated. We would like to thank you very much for your support.
Can Vuran
I do appreciate for your service including submission, analysis, review, editorial and publishing process. I believe these esteemed journal enlighten the science with its high-quality personel.
Bora Uysal
I am very much pleased with the fast track publication by your reputed journal's editorial team. It is really helpful for researchers like me from developing nations. I strongly recommend your journal for publication.
Badri Kumar Gupta
It has been a fabulous journey writing articles for your journal because of the encouragement you people provide for writers from developing nations like India. Kindly continue the same. Looking forward for a long term association.
Badareesh Lakshminarayana
Many thanks for publishing my article in your great journal and the friendly and hassle-free publication process, the constructive peer-review, the regular feedback system, and the Quick response to any queries.
Azab Elsayed Azab
I would like to thank this journal for publishing my Research Article. Something I really appreciate about this journal is, they did not take much time from the day of Submission to the publishing date. Looking forward to have more publications in future.
Ayush Chandra
Submission of paper was smooth, the review process was fast. I had excellent communication and on time response from the editor.
Ayokunle Dada
Your service is very good and fast reply, also your service understand our situation and support us to publication our articles.
Ayman M Abu Mustafa
Really good service with prompt response. Looking forward to having long lasting relationship with your journal
Avishek Bagchi
Your service is excellent. Processing and editing were very fast. I hope to publish more of my works in your journal.
Ausraful Islam
I wanna to thank Clinical Journal of Nursing Care and Practice for its effort to review and publish my manuscript. This is reputable journal. Thank you!
Atsedemariam Andualem
“It was a delightful experience publishing my manuscript with the Clinical Journal of Obstetrics and Gynecology. They offered me lots of opportunities I never had from most publishing houses and their prompt services are greatly appreciated.”
Asafo Jones
I hope to ability to make some new investigation and publish in Your Company in future.
Artur Stopyra
I like the quality of the print & overall service. The paper looks quite impressive. Hope this will attract interested readers. All of you have our best wishes for continued success.
Arshad Khan
Your big support from researchers around the world is the best appreciation from your scientific teams. We believe that there should be no barrier in science and you make it real and this motto come true.
Arefhosseinir Rafi
Your journal co-operation is very appreciable and motivational. I am really thankful to your journal and team members for the motivation and collaboration to publish my work.
Assistant Professor, UCLAS Uttaranchal University, Dehradun, India
Archna Dhasmana
I am glad to submit the article to Heighten Science Publications as it has a very smooth and fast peer-review process, which enables the researchers to communicate their work on time.
Anupam M
This is to specify that I have had an extensive and detailed interaction with the Editorial team of Annals of Clinical Gastroenterology and Hepatology, USA, lasting over a significant period of time. My interaction has been extremely pleasant, especially with Ms Allie Smith, as I find the communication quite inspiring and crystal clear. The attitude of aforesaid individuals is quite helpful and guiding in pertinent instances. It has been a commemorative journey so far working with the Journal and I hope that the symbiosis will continue, evolve and flourish in the forthcoming years. I wish the journal, related personnel and aforementioned individuals a fruitful, successful run.
New Delhi, India
Anubha Bajaj
We appreciate the fact that you decided to give us full waiver for the applicable charges and approve the final version. You did an excellent job preparing the PDF version. Of course we will consider your magazine for our future submissions and we will pay the applicable fees then.
Anna Dionysopoulou
''Co-operation of Archives of Surgery and Clinical Research journal is appreciable. I'm impressed at the promptness of the publishing staff and the professionalism displayed. Thank you very much for your support, help and encouragement.''
Anıl Gokce
Congratulations for the excellence of your journal and high quality of its publications.
Angel MARTIN CASTELLANOS
The service from the journal staff has been excellent.
Andy Smith
I was very pleased with the quick editorial process. We are sure that our paper will have great visibility, among other things due to its open access. We believe in science accessible to all.
Anderson Fernando de Souza
It was a great experience publishing through JCICM. The article has reached out to several institutions. Appreciate your professional work. Hope to work with you again
Anas Wardeh
Publishing an article is a long process, but working with your publication department made things go smoothly, even though the process took exactly 5 months from the time of submitting the article till the time I have favourable response, the missing part is the peer review details, which is essential in self auditing and future improvement, overall experience was excellent giving your understanding of the situation of lack of financial institution support.
Anas Diab
I think that Heighpubs very good. You are very helpful. Thank you for everything.
Ana Ribeiro
Regarding to be services, we note that are work with high standards of professionalism translated into quick response, efficiency which makes communication accessible. Furthermore, I believe to be much inviting for the submission of future works for publication purposes.
Amélia João Alice Nkutxi
I would like to mention that I had a wonderful experience working with HSPI. The whole process right from manuscript submission to peer review till the publication of the article was very prompt & efficient. I wish you good luck for the future.
Amarjeet Gambhir
Once I submitted the manuscript, the response time of the reviewers was very fast. The fine-tuning of the galley proof was likewise prompt. I believe the journal provide a valuable outlet to disseminate physical rehabilitation scientific knowledge to the clinical community. Respectfully. Dr. Alon
Alon
We really appreciate and thanks the full waiver you provide for our article. We happy to publish our paper in your journal. Thank you very much for your good support and services.
Ali Abusafia
It was a real pleasure working with your team. The review was done fast, and it was very clear, the editing was flawless, the article was published quickly compared to other journals, and everyone was understanding and helpful. I will gladly recommend this journal to my acquaintances in academia.
Alexandra Cozma
To the editorial team at HSPI and the Journal of Clinical Nephrology: Thank you so much for your hard work and collaboration in bringing our article to life. Your staff was responsive, flexible, and communicative and made the process smooth and easy. Thank you!
Alejandro Munoz
Dear colleagues! I am satisfied with our cooperation with you. Your service is at a high level. I hope for a future relationship. Let me know if I can get a paper version of the magazine with my articles from you. I see them on the Internet.
Aksenov V.V
"This is my first time publishing with the journal/publisher. I am impressed at the promptness of the publishing staff and the professionalism displayed. Thank you for encouraging young researchers like me!"
Ajite Kayode
I want to thank you for our collaboration. You were fast and effective with a positive spirit of teamwork. I am truly excited from our collaboration. You were like always fast, efficient and accurate. I hope that in the near future we will collaborate again.
Aikaterini Solomou
In my opinion, you provide a very fast and practical service.
Ahmet Eroglu
Great, We are too comfortable with the process including the peer review process and quality. But, the journal should be indexed in different databases such scopus.
Afework Edmealem
We really appreciate your efforts towards our article, the professional way you handle our request for exemption from charges. It was a great honor for us to publish in your magazine.
Achraf elbakkaly
I really liked the ease of submitting my manuscript in the HSPI journal. Further, the peer review was timely completed and I was communicated the final decision on my manuscript within 10 days of submission which is really appreciable. I strongly recommend all the scientists and researchers to submit their work in this journal”
Abu Bashar
My candid opinion is that the service you render is second to none. My favourite part is the prompt response to issue, really i value that.
Abiodun Akanbi Adeogun
Thank you very much for accepting our manuscript in your journal “International Journal of Clinical Virology”. We are very thankful to the esteemed team for timely response and quick review process. The editorial team of International Journal of Clinical Virology is too cooperative and well-mannered during the publication process. We are hopeful to publish many quality papers in your journal and I suggest the International Journal of Clinical Virology to all of my colleagues, researchers and friends to publish their research here.
Abdul Baset
I, Muhammad Sarwar Khan, am serving as Editor on Archives of Biotechnology and Biomedicine (ABB). I submitted an editorial titled, 'Edible vaccines to combat Infectious Bursal Disease of poultry' for publication in ABB. After submitting the manuscript; the services rendered by the management and technical personnel to handle and process the manuscript were marvelous. Plagiarism report was shared with me with complements before reviewers' comments, All steps including article processing and service charges were well taken care of keeping in view the author's interest/preference. All together, it was an encouraging and wonderful experience working with ABB personnel.
University of Agriculture, Pakistan
Muhammad Sarwar Khan
Your journal has accomplished its intended mission of providing very effective and efficient goals in dealing with submissions, conducting the reviewing process and in publishing accepted manuscripts in a timely manner. Keep up the great work and services that you provide.
University of Jacqmar, Inc., USA
John St. Cyr
I am to express my view that Heighten Science Publications are reliable quick even after peer review process. I hope and wish the publications will go a long way in disseminating science to many interested in scientific research.
College of Fisheries, CAU(I), Tripura, India
Ajit Kumar Roy
The Journal Clinical Nephrology provides a good opportunity for readers to stay updated in the field of clinical nephrology. Additionally - it provides a good opportunity for authors to publish their work. 1. Publication of the accepted manuscripts is sufficiently rapid. 2. The trust factor between the journal and me, as an author, is very important and well preserved. 3. Peer review process very rapid and effective.
Assaf Harofeh Medical Center, Israel
Leonid Feldman
In 2017, I submitted a manuscript to the journal Archives of Biotechnology and Biomedicine belonging to Heighten Science Publications Corporation. Within one week I already received the response from the editor. All processing steps were really fast so in terms of a speedy publication I can particularly recommend the journal Archives of Biotechnology and Biomedicine. The responsible contact person of the journal was always available, which gives a trustworthy impression to the author. Also the peer review process was clear and constructive. So from my experience with Heighten Science Publications Corporation I can recommend publishing there.
University of Tubingen, Germany
Yvonne Mast
We thank to the heighten science family, who speed up the publication of our article and provide every support.
Mehmet Besir
The services of the journal were excellent. The most important thing for an author is the speed of the peer review which was really fast here. They returned in a few days and immediately replied all of my questions. I want to refer this platform to all scholars. Many thanks.
Eastern Mediterranean University, Cyprus
Zehra Guchan TOPCU
Thank you for your attitude and support. I am sincerely grateful to you and the entire staff of the magazine for the high professionalism and fast quality work. Thank you very much!
USA
Igor Klepikov
Thank you and your company for effective support of authors which are very much dependable on the funds gambling for science in the different countries of our huge and unpredictable world. We are doing our work and should rely on a teams like Galley Proof-HSPC. Great success to all of you for the 2019th! Be well all the year long.
Russia
Victor V Apollonov
The editorial process was quickly done. The galley proof was sent within a week after being accepted for publication. The editorial team was very helpful and responded promptly.
India
Rohit Kulshrestha
Publishing with the International Journal of Clinical and Experimental Ophthalmology was a rewarding experience as review process was thorough and brisk. Their visibility online is second to none as their published articles appear in all search engines. I will encourage researchers to publish with them.
University of Port Harcourt Teaching Hospital, Nigeria
Dr. Elizabeth A Awoyesuku
"It was a pleasure to work with the editorial team of the journal on the submission of the manuscript. The team was professional, fast, and to the point".
NC A&T State University, USA
Moran Sciamama-Saghiv
Submission of paper was smooth, the review process was fast. I had excellent communication and on time response from the editor.
Ekiti State University Teaching Hospital, Nigeria
Ayokunle Dada
I am delighted and satisfied with. Heighten Science Publications as my manuscript was thoroughly assessed and published on time without delay. Keep up the good work.
Ido-Ekiti/Afe Babalola University, Nigeria
Dr. Shuaib Kayode Aremu
"This is my first time publishing with the journal/publisher. I am impressed at the promptness of the publishing staff and the professionalism displayed. Thank you for encouraging young researchers like me!"
Ekiti State University, Nigeria
Adebukola Ajite
I wanna to thank clinical journal of nursing care and practice for its effort to review and publish my manuscript. This is reputable journal. Thank you!
Wollo University, Ethiopia
Atsedemariam Andualem
We appreciate your approach to scholars and will encourage you to collaborate with your organization, which includes interesting and different medical journals. With the best wishes of success, creativity and joy in life, prosperity in the medical field.
Ivano- Frankivsk National Medical University, Ukraine
Nataliya Kitsera
Thank you very much for your support and encouragement. I am truly impressed by your tolerance and support. Thank you very much
Diaverum: PADC, Jeddah, Saudi Arabia
Nasrulla Abutaleb
You are such a nice person. Your journal co-operation is very appreciable and motivational.
Department of Biotechnology, Uttaranchal college of Applied and Life Sciences, Uttaranchal University, Dehradun, Uttarakhand, India
Archna Dhasmana
“Mobile apps and wearable technology are becoming ubiquitous in our environment. Their integration with healthcare delivery is just beginning to take shape. The early results are promising and the possibilities great."
BS, PharmD., MBA, CPHIMS, FHIMSS, Adjunct Professor, Global Healthcare Management, MCPHS University, Chief Strategy Offi cer, MedicaSoft, Senior Advisor, National Health IT (NHIT) Collaborative for Underserved, New York HIMSS, National Liaison, Health 2.0 Boston, Past Chair, Chair Innovation, USA
Helen Figge
“The choice to submit the forensic case study to the Journal of Addiction Therapy and Research was dictated by the match between the content and the potential readership. The publication process proved to be expedient and we were provided with constructive feedback from reviewers. The final article layout is attractive and conforms to standards. All-in-all, it has been a rewarding process.”
Ph.D, Boston University Department of Communication Sciences and Disorders and Knowledge Research Institute, Inc., 2131 Reflection Bay Drive, Arlington, Texas 76013, USA
Elisabeth H. Wiig
The service is nice and the time of processing the application is fast.
Department of Neurosurgery, Queen Elizabeth Hospital, Hong Kong
Long Ching
Your service is very good and fast reply, Also your service understand our situation and support us to publication our articles.
Palestine College of Nursing, Khan Younis, Gaza Strip, Palestine
Ayman M Abu Mustafa
“It was a delightful experience publishing my manuscript with the Clinical Journal of Obstetrics and Gynecology. They offered me lots of opportunities I never had from most publishing houses and their prompt services are greatly appreciated.”
Department of Agricultural Economics, Agribusiness and Extension, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana
Akowuah Jones Asafo
Related Journals

HSPI: We're glad you're here. Please click "create a new Query" if you are a new visitor to our website and need further information from us.
If you are already a member of our network and need to keep track of any developments regarding a question you have already submitted, click "take me to my Query."